Dopplerometry during pregnancy is a modern diagnostic method using ultrasound, which allows you to objectively and fully examine the blood circulation of the fetus, placenta and uterus. Based on the state of the circulatory system, you can assess the condition of the fetus, the speed of its development - whether the baby is suffering from a lack of oxygen, as well as possible pathological changes. Fetal Doppler is the only technique that can show the exact location of vascular pathology (in the uterus, umbilical cord or placenta).
Consultation with a doctor based on test results or ultrasound - 500 rubles. (at the patient's request)
Why and when to do Doppler testing during pregnancy
Today, vascular diseases are one of the most common problems in medical practice. Timely diagnosis makes it possible to identify such pathologies at an early stage of development, and at the same time many factors that can cause the development of circulatory disorders.
The value of the procedure lies in its high information content, thanks to which the doctor is able to identify not only already developed pathology, but also almost imperceptible preclinical symptoms of the disease. The procedure is prescribed after the placenta is fully formed - no earlier than 18 weeks, most often at 32-34 weeks as a routine check.
If there is even a slight suspicion of fetal developmental disorders, an ultrasound with Doppler is performed at any stage. Doppler is done in combination with , while for a pregnant woman the procedure feels no different from a classic ultrasound examination.
The essence of the method
This method of studying the circulatory system is based on the use of the Doppler effect.
The examination uses the same ultrasound as in a conventional ultrasound examination. The difference lies in a special sensor based on the Doppler effect and the interpretation of the data obtained. During the study, ultrasonic waves are recorded, reflected not from static tissues, but from moving objects - blood cells, as a result of which the frequency of the reflected rays changes greatly in comparison with those being studied. The device processes the received data and creates a two-dimensional color image. Thanks to this, it is possible to assess the speed and direction of blood flow, the anatomy and patency of blood vessels.
The duration of Doppler ultrasound is 20 – 40 minutes. It has no contraindications, no complications, no negative effects on the body. The examination is completely painless and safe.
Indications
Gynecologists recommend undergoing Doppler examination 1-2 times during pregnancy along with . If there are problems, fetal doppler testing should be done as soon as possible. Basically, Doppler testing is prescribed when the size of the fetus does not correspond to its gestational age. The procedure is also carried out in the following cases:
- complications in bearing a child;
- fetoplacental insufficiency;
- the mother has chronic and severe diseases (diabetes mellitus, hypertension, anemia, systemic diseases);
- Rh conflict between pregnant woman and child;
- multiple pregnancy;
- non-immune hydrops fetalis;
- incorrect position of the fetus in the uterus;
- premature maturation of the placenta;
- umbilical cord entwined around the child’s neck, suspected hypoxia;
- severe oligohydramnios/polyhydramnios;
- gestosis (late toxicosis, accompanied by deterioration of the kidneys, blood vessels and brain - protein appears in the urine, pressure increases);
- injuries pregnant woman's belly;
- chromosomal pathologies of the baby;
- the fetus moves less than usual or no movement is felt at all;
- unsatisfactory results of cardiotocography;
- complications in carrying a previous pregnancy (premature birth, miscarriage, etc.).
Also, a fetal ultrasound with Doppler should be performed in cases where the mother is under 20 years old or she is over 35 years old.
What does fetal Doppler sonography reveal?
Doppler helps to promptly detect fetal hypoxia and avoid the problem even before the child is in danger, or reduce negative consequences to a minimum. With its help, the doctor can find out the reasons for the umbilical cord entanglement and see how many times and how tightly the baby’s neck is entwined. Without this vital information, specialists will not be able to choose the right delivery tactics, which jeopardizes the health and life of the child.
You can also see with the help of Doppler:
- the state and rhythm of the fetal heart in a state of rest and movement;
- the condition of the heart valves of the main blood vessels, arteries and veins;
- speed and volume of blood flow of the peripheral circulatory system;
- blood circulation in the umbilical cord and placenta;
- condition of the circulatory system, heart and kidneys of the pregnant woman.
The information obtained allows the doctor to assess:
- patency and condition of the vascular bed, the presence of abnormalities blocking fetal blood flow;
- saturation of all tissues of the child with blood and nutrients;
- patency and condition of the umbilical cord, entanglement of the baby’s neck;
- efficiency of the placenta;
- the condition and functioning of a woman’s circulatory system during pregnancy.

Preparation and features of fetal ultrasound with Doppler
The procedure does not require any preparatory measures: neither the diet nor the fullness of the bladder and stomach affect the examination results. The only recommendation is to take a break from eating for a couple of hours before the examination.
A pregnant woman needs to take with her the following: directions and results of past tests and examinations (ultrasound, CTG, ECG), a pregnant woman’s exchange card. Paper napkins and a disposable diaper or towel are not needed - everything is provided free of charge in our clinic.
The technique of Doppler ultrasound is similar to transabdominal ultrasound. The woman lies down on the couch with her back and exposes her stomach. The doctor applies a special gel to the area under study to improve the passage of ultrasonic waves and then moves the sensor along it, while simultaneously examining the data obtained on the monitor. An interpretation of the results is given to the woman on the same day.
Doppler measurements during pregnancy can be carried out in several ways:
- Doppler ultrasound is used to assess the direction, intensity, and nature of blood flow in the vessels.
- Duplex research differs from the previous method in being more accurate and informative. Used to assess vascular blood flow and their anatomy.
- Color mapping – the condition of even the smallest vessels and their patency is color coded.
Interpretation of fetal Doppler results
Assessment of the state of blood supply using Doppler is based on the following indicators:
- Systole-diastolic ratio is the ratio of maximum and minimum blood flow speed;
- Index resistance - the ratio of the difference between the maximum and minimum blood flow speeds to the maximum during the compression period;
- Pulsating index – the ratio of the difference between the maximum and minimum blood flow speed to the average speed for a full cardiac cycle.
Fetal Doppler: weekly norm and prognosis for deviations
In order for the results to be deciphered correctly and all deviations to be identified, it is necessary to compare the data obtained with standard values, taking into account the gestational age.

Indicators of the norm of the uterine artery resistance index
Gestational period (weeks) | Average IR of the uterine arteries | Possible range of fluctuations |
0,52 | 0,37 – 0,7 |
|
0,51 | 0,36 – 0,69 |
|
0,36 – 0,68 |
||
0,36 – 0,68 |
||
0,35 – 0,67 |
||
0,49 | 0,35 – 0,66 |
|
0,49 | 0,35 – 0,65 |
|
0,48 | 0,34 – 0,64 |
|
0,48 | 0,34 – 0,64 |
|
0,47 | 0,34 – 0,63 |
|
0,46 | 0,34 – 0,62 |
|
0,46 | 0,34 – 0,61 |
|
0,45 | 0,34 – 0,61 |
|
0,45 | 0,34 – 0,59 |
|
0,45 | 0,34 – 0,59 |
|
0,45 | 0,33 – 0,58 |
|
0,44 | 0,33 – 0,58 |
|
0,44 | 0,33 – 0,57 |
|
0,44 | 0,33 – 0,57 |
|
0,43 | 0,33 – 0,57 |
|
0,43 | 0,32 – 0,57 |
|
0,43 | 0,32 – 0,56 |
Standard indicators of the pulsatility index of the uterine arteries
Gestational period (weeks) | Average PI of the uterine arteries | Possible range of fluctuations |
1,54 | 1,04 – 2,03 |
|
1,47 | 0,98 – 1,96 |
|
1,41 | 0,92 – 1,9 |
|
1,35 | 0,86 – 1,85 |
|
0,81 – 1,79 |
||
1,25 | 0,76 – 1,74 |
|
0,71 – 1,69 |
||
1,16 | 0,67 – 1,65 |
|
1,12 | 0,63 – 1,61 |
|
1,08 | 0,59 – 1,57 |
|
1,05 | 0,56 – 1,54 |
|
1,02 | 0,53 – 1,51 |
|
0,99 | 0,5 – 1,48 |
|
0,97 | 0,48 – 1,46 |
|
0,95 | 0,46 – 1,44 |
|
0,94 | 0,44 – 1,43 |
|
0,92 | 0,43 – 1,42 |
|
0,92 | 0,42 – 1,41 |
|
0,91 | 0,42 – 1,4 |
|
0,91 | 0,42 – 1,4 |
|
0,91 | 0,42 – 1,4 |
|
0,92 | 0,42 – 1,41 |
Indicators of the right and left uterine artery may be different. The main thing is that both indicators do not go beyond the norm. If both indicators are not normal, this indicates a violation of the uteroplacental circulation. If one indicator is for asymmetry of uteroplacental blood flow
It is important to note that at 18-21 weeks, deviations in indicators may be observed due to the incomplete adaptive physiological process of cytotrophoblast invasion. In this case, Doppler testing of the fetus should be repeated after 2-3 weeks.
Standard indicators of the systole-diastolic ratio in the fallopian tubes
Normal Doppler measurement: umbilical cord arteries
Standard values of the umbilical cord artery resistance index:
Gestational period (weeks) | Average index of IR of the umbilical cord arteries | Possible range of fluctuations |
0,74 | 0,63 – 0,84 |
|
0,73 | 0,62 – 0,83 |
|
0,72 | 0,61 – 0,82 |
|
0,71 | 0,6 – 0,82 |
|
0,59 – 0,81 |
||
0,69 | 0,58 – 0,8 |
|
0,68 | 0,58 – 0,79 |
|
0,67 | 0,57 – 0,79 |
|
0,66 | 0,56 – 0,78 |
|
0,65 | 0,55 – 0,78 |
|
0,64 | 0,54 – 0,77 |
|
0,63 | 0,53 – 0,76 |
|
0,62 | 0,52 – 0,75 |
|
0,61 | 0,51 – 0,74 |
|
0,49 – 0,73 |
||
0,59 | 0,48 – 0,72 |
|
0,58 | 0,46 – 0,71 |
|
0,57 | 0,44 – 0,7 |
|
0,56 | 0,43 – 0,69 |
|
0,55 | 0,42 – 0,68 |
|
0,54 | 0,41 – 0,67 |
|
0,53 | 0,4 – 0,66 |
Standard values of the pulsatility index of the umbilical cord arteries:
Gestational period (weeks) | Average PI of the umbilical cord arteries | Possible range of fluctuations |
1,72 | 1,53 – 1,9 |
|
1,62 | 1,45 – 1,78 |
|
1,45 | 1,25 – 1,65 |
|
1,35 | 1,18 – 1,51 |
|
1,35 | 1,17 – 1,52 |
|
1,25 | 1,09 – 1,41 |
|
1,12 | 0,96 – 1,27 |
|
1,15 | 0,98 – 1,33 |
|
1,01 | 0,86 – 1,16 |
|
1,01 | 0,86 – 1,16 |
|
1,05 | 0,87 – 1,23 |
|
1,03 | 0,88 – 1,17 |
|
0,95 | 0,76 – 1,13 |
|
0,85 | 0,71 – 0,99 |
|
0,84 | 0,67 – 1,1 |
|
0,84 | 0,59 – 0,93 |
|
0,83 | 0,58 – 0,99 |
|
35 — 37 | 0,81 | 0,57 – 1,05 |
38 — 41 | 0,74 | 0,37 – 1,08 |
Obtaining zero and reverse values of diastolic blood flow is considered a pathology. This indicates a critical condition of the fetus, the death of which will occur in 2-3 days. In this case, a cesarean section is immediately prescribed (if the gestational age is more than 28 weeks) to save the baby's life.
Standard values for the systole-diastolic ratio of the umbilical cord arteries:
Impaired blood flow in the umbilical cord entails a delay in the development of the child.
Doppler ultrasound norms: middle cerebral artery of the fetus
Gestational period (weeks) | Average PI in the middle cerebral artery | Possible range of fluctuations |
1,83 | 1,36 – 2,31 |
|
1,87 | 1,4 – 2,34 |
|
1,91 | 1,44 – 2,37 |
|
1,93 | 1,47 – 2,4 |
|
1,96 | 1,49 – 2,42 |
|
1,97 | 1,51 – 2,44 |
|
1,98 | 1,52 – 2,45 |
|
1,99 | 1,53 – 2,45 |
|
1,99 | 1,53 – 2,46 |
|
1,99 | 1,53 – 2,45 |
|
1,98 | 1,52 – 2,44 |
|
1,97 | 1,51 – 2,43 |
|
1,95 | 1,49 – 2,41 |
|
1,93 | 1,46 – 2,39 |
|
1,43 – 2,36 |
||
1,86 | 1,4 – 2,32 |
|
1,82 | 1,36 – 2,28 |
|
1,78 | 1,32 – 2,24 |
|
1,73 | 1,27 – 2,19 |
|
1,67 | 1,21 – 2,14 |
|
1,61 | 1,15 – 2,08 |
|
1,55 | 1,08 – 2,01 |
Maximum velocity in the fetal middle cerebral artery:
Gestational period (weeks) | Average indicator | Possible range of fluctuations |
19,7 | 16,7 – 23 |
|
21,8 | 18,1 — 26 |
|
23,9 | 19,5 — 29 |
|
20,8 — 32 |
||
28,2 | 22,2 – 35 |
|
30,3 | 23,6 – 38,1 |
|
32,4 | 24,9 – 41,1 |
|
34,6 | 26,3 – 44,1 |
|
36,7 | 27,7 – 47,1 |
|
38,8 | 29 – 50,1 |
|
40,9 | 30,4 – 53,1 |
|
43,1 | 31,8 – 56,1 |
|
45,2 | 33,1 – 59,1 |
|
47,3 | 34,5 – 62,1 |
|
49,5 | 35,9 – 65,1 |
|
51,6 | 37,2 – 68,2 |
|
53,7 | 38,6 – 71,2 |
|
55,8 | 40 – 74,2 |
|
41,3 – 77,2 |
||
60,1 | 42,7 – 80,2 |
|
62,2 | 44,1 – 83,2 |
|
64,4 | 45,4 – 86,2 |
Standard values of the systolic-diastolic ratio in the middle cerebral artery:
Normal fetal Doppler findings: fetal aorta
Disturbances in the blood circulation of the fetal aorta can be detected only after 22-24 weeks of pregnancy.
Standard values of the pulsatility index of the fetal aorta:
Gestational period (weeks) | Average PI of the fetal aorta | Possible range of fluctuations |
1,79 | 1,49 – 2,16 |
|
1,79 | 1,49 – 2,16 |
|
1,79 | 1,49 – 2,17 |
|
1,49 – 2,18 |
||
1,49 – 2,19 |
||
1,81 | 1,49 – 2,2 |
|
1,81 | 1,49 – 2,21 |
|
1,82 | 1,5 – 2,22 |
|
1,83 | 1,5 – 2,24 |
|
1,82 | 1,51 – 2,25 |
|
1,81 | 1,51 – 2,26 |
|
1,81 | 1,52 – 2,28 |
|
1,53 – 2,29 |
||
1,53 – 2,31 |
||
1,79 | 1,54 – 2,32 |
|
1,79 | 1,55 – 2,34 |
|
1,79 | 1,55 – 2,35 |
|
1,92 | 1,56 – 2,36 |
|
1,93 | 1,57 – 2,38 |
|
1,94 | 1,57 – 2,39 |
|
1,94 | 1,57 – 2,4 |
|
1,95 | 1,58 – 2,41 |
Standard values of the fetal aortic resistance index:
Standard values for fetal aortic systolic velocity:
Gestational period (weeks) | Average systolic velocity | Possible range of fluctuations |
26,88 | 12,27 – 44,11 |
|
28,87 | 14,1 – 46,28 |
|
30,52 | 15,6 – 48,12 |
|
31,95 | 16,87 – 49,74 |
|
33,23 | 18 – 51, 2 |
|
34,39 | 19 – 52,55 |
|
35,47 | 19,92 – 53,81 |
|
36,47 | 20,77 – 55,01 |
|
37,42 | 21,55 – 56,13 |
|
38,32 | 22,3 – 57,22 |
|
39,17 | 23,02 – 58,26 |
|
40,01 | 23,66 – 59,27 |
|
40,8 | 24,3 – 60,26 |
|
41,57 | 24,92 – 61,21 |
|
42,32 | 25,52 – 62,16 |
|
43,06 | 26,1 – 63,08 |
|
43,79 | 26,67 – 64,02 |
|
44,52 | 27,24 – 64,93 |
|
45,24 | 27,8 – 65,81 |
|
45,96 | 28,37 – 66,72 |
|
46,7 | 28,95 – 67,65 |
|
47,47 | 29,57 – 68,62 |
Standard values for the systolic-diastolic ratio of the fetal aorta:
Doppler norms during pregnancy: ductus venosus
The ductus venosus is not assessed using indices. An indicator of pathology is zero or negative blood flow values. Typically, similar values are obtained for fetal malnutrition, congenital heart disease, and nonimmune hydrops.
In the case when the blood circulation in the umbilical cord is in a critical condition, but no blood flow deviations were detected in the venous duct, it is possible to extend gestation until the optimal period for delivery.
How will a gynecologist understand whether there is fetal hypoxia?
The doctor compares normal Doppler measurements with the result obtained.
- An increase in IR and SDO in the uterine arteries is a sign that the baby is not receiving enough oxygen. This will lead to developmental delays.
- An increase in Doppler readings for the umbilical cord artery is a sign of feto-placental insufficiency. This is a vascular pathology, so the fetus is already suffering. This is also a sign of gestosis.
- If the indicators of IR and SDO in the umbilical cords differ during multiple pregnancy, this indicates that one of the babies is experiencing hypoxia (transfusion syndrome).
- Excess of SDO and IR in the aorta is a symptom of poor health of the child due to post-term pregnancy, due to diabetes mellitus in the pregnant woman, in case of a conflict regarding the Rh factor, etc.
- A decrease in SDO and IR during Doppler measurements in the carotid and cerebral arteries is observed in extremely severe conditions of the fetus, since in this case only the main organs that support life are supplied with blood. In such a situation, artificial childbirth must be performed immediately.
Over the past decade, medical institutions have been widely equipped with ultrasound scanners equipped with color Doppler mapping and reducing the total radiation exposure to the fetus to a safe threshold. This makes it possible to expand the scope of standard screening ultrasound examination of pregnant women for the early formation of high-risk groups. Among the Doppler parameters determined in the first trimester of pregnancy, the study of blood flow velocity curves (BVR) in the fetal venous duct has attracted the greatest attention of researchers. The high prognostic value of studying the spectrum of CSCs in this vessel at the end of the first – beginning of the second trimester of pregnancy has been proven in relation to the presence of chromosomal abnormalities, congenital heart defects in the fetus and the outcome of multiple pregnancies. But these studies concerned only the qualitative study of CSC (registration of retrograde or unidirectional blood flow). Quantitative normative parameters of blood flow velocity in the fetal venous duct at the turn of the first and second trimesters of pregnancy in various phases of the cardiac cycle still remain unknown. This limits the possibility of using this method to predict other types of obstetric pathology. The existing problem indicated the direction of the research.
The purpose of the work is to determine the normative parameters of fetal blood flow rates in 11–14 weeks of pregnancy.
Material and research methods
The subject of the study consisted of 72 somatically healthy women with a physiological course of singleton pregnancy, having from 11 weeks. + 0/7 days up to 13 weeks. + 6/7 days of gestation. Criteria for inclusion in the study:
a) age from 18 to 35 years;
b) pregnancy from 11 to 14 weeks;
c) bearing one fetus;
d) the location of the chorion in the fundus or along the side walls of the uterus;
e) absence of extragenital pathology in the stage of sub- and decompensation;
f) spontaneous conception;
g) the absence of an episode of threatening termination of the observed pregnancy both at the time of the study and at its earlier stages.
The study of blood circulation in the fetal venous duct was carried out using a Voluson E8 ultrasound device (USA), in compliance with the ALARA (As Low As Reasonably Achievable) principle - “As Low As Reasonably Achievable”, i.e. using the most prudently low output power possible. Registration of blood flow in the fetal venous duct was carried out by specialists who have the appropriate Certificate from the Fetal Medicine Foundation. The velocity of blood flow was measured in systole (S), diastole (E) of the ventricles of the heart, as well as during contraction of the vestibules of the heart, i.e. in late diastole (A).
The ratios of phase blood flow velocities (S/E and S/A), as well as angle-independent indices - venous resistance index (VRI) and venous velocity index (VVI) were calculated. The study was conducted as an addition to the standard examination in the first trimester of pregnancy, determined by the “Basic spectrum of examination of pregnant women” of the federal Procedure for the provision of medical care in the field of “obstetrics and gynecology (except for the use of assisted reproductive technologies)”. In addition to the data from the clinical examination of patients, the work took into account the content of pregnancy-related plasma protein A (PAPP-A) and the free beta subunit of human chorionic gonadotropin (beta-hCG) in the blood of women on the day of examination, both in quantitative values and in the form of “multiple” of median" (MoM).
The recorded data were processed using the method of correlation and variation analysis and are presented as “mean ± standard deviation” (M ± SD) and 95% confidence interval (95% CI).
Research results and discussion
The data obtained indicate that the speed of blood flow in the ductus venosus in the fetus at the turn of the first and second trimesters of gestation during a physiological pregnancy varies widely (table).
In various phases of the fetal cardiac cycle, individual characteristics in the group of subjects determined a more than twofold discrepancy in the recorded parameters. At the same time, the linear parameters of blood circulation did not depend on either the gestational age in weeks or the thickness of the chorion measured by ultrasound scanning. There were no cases of retrograde blood flow in the ductus venosus in the fetus (a marker of intrauterine hypoxia or hereditary pathology) in the examined women.
Indicators of blood flow velocity curves in the fetal ductus venosus in various phases of the cardiac cycle in the early stages of physiological pregnancy
Blood flow in the ductus venosus
During the entire period of intrauterine development, the embryo, and later the fetus, is affected by various harmful factors. In such conditions, the young mother has a serious responsibility: on the one hand, to protect the baby from external threats:
And on the other hand, to ensure the internal constancy of the body. The healthcare system provides a gentle daily regimen (including physical activity) for a pregnant woman. The relevance of the issue is due to the fact that the slightest provoking factors can affect the baby’s health. Already today, according to WHO, there is an increase in the number of newborns with developmental anomalies in urbanized cities.
In this case, it is recommended to carry out timely screening. An innovator in this area is the Minimax company, which is engaged in research in all areas of medicine. Back in 1994, the company conducted Doppler studies, and now these technologies make it possible to detect intrauterine anomalies in the early stages.
Venous blood flow: research methods
Of greatest interest from the point of view of identifying anomalies is the blood flow in the ductus venosus, as well as the umbilical artery. The ductus venosus (Ductus of Arantius) is a narrow canal connecting the umbilical and inferior vena cava. This is essentially an anastomosis that bypasses the hepatic bloodstream. The feasibility of studying the speed of blood flow, as well as its direction, arises already in the early stages of fetal development.
Already at 11 weeks, the first ultrasound examinations are performed: normally, blood flow in the ductus venosus in the fetus should move towards the right atrium. Often, genetic characteristics, as well as teratogenic factors, lead to the fact that the fetus has critical (sometimes incompatible with life) developmental anomalies.
One of the most popular problems is reverse venous blood flow. In this case, peaks are recorded on ultrasound, which indicate blood is being discharged in the opposite direction (to the umbilical vein). This may indicate tricuspid valve insufficiency or other cardiovascular abnormalities.
If the venous blood flow of the fetus is disrupted and intrauterine development is not threatened, then surgical interventions are performed after birth.
Reverse blood flow in the ductus venosus in the fetus. How should we treat him?
At the first ultrasound screening a week ago, the sonologist discovered something incomprehensible, which he called “reverse blood flow in the ductus venosus in the fetus.” These words make your hair stand on end, and the worst thoughts take root in your head. It seems that life has stopped, and what you hear is nothing more than a sentence. But in order to take a thoughtful and balanced step, let's figure it out without emotions.
What is ductus venosus reversal in the fetus?
The ductus venosus is a vessel that connects the umbilical vein (which carries oxygenated arterial blood) with the inferior vena cava. It has a very small diameter - only 2-3 mm, so only an experienced sonologist is able to examine it, and then only with expert-class equipment. Through the venous duct, arterial blood immediately enters the heart and partially into the brain, because It is these organs that need large amounts of oxygen.
The blood flow in this vessel is normally directed only in one direction (towards the heart). Reverse flow is not possible due to the powerful smooth muscle sphincter present in the venous duct. However, under certain conditions, the pressure in the vessel increases so much that a reversal of the ductus venosus appears in the fetus, i.e. movement of blood in the opposite direction (away from the heart).
What does reverse blood flow look like in the ductus venosus in the fetus?
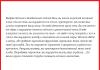
Normally, the Dopplerographic picture of the venous duct is three-phase (see Figure 1):
- Contraction of the ventricles. At this time, the atria are maximally relaxed, so blood flows to them at a very high speed. This is the highest peak on the graph (labeled “A” in the figure).
- Passive filling of the ventricles from the atria (early diastole). The blood flow speed is also high, but somewhat less than in systole. Therefore, on the graph this is a peak of lower height (indicated by the letter “B”).
- Atrial contraction and active filling of the ventricles. The movement of blood slows down sharply, so a notch appears (indicated by the letter “C”), but normally it never reaches the zero line because the blood in the ductus venosus does not move back.
Figure 1. Normal blood flow in the ductus venosus
If a reverse of the ductus venosus appears in the fetus, this indicates that the pressure in the vessel is very high, and the blood rushes in the opposite direction at the moment of atrial contraction. In the ultrasound picture it looks like this (see Figure 2). Below the isoline, a wave is determined (indicated by a circle).
Figure 2. Reversal of blood flow in the ductus venosus in the fetus.
What does reverse in the ductus venosus in the fetus indicate?
Reversal in the ductus venosus is considered a marker of chromosomal pathology or heart disease in the fetus, reflecting hemodynamic insufficiency. However, this feature cannot be absolutized either. In a study of high-risk patients, it was found that reverse blood flow in the fetal ductus venosus was associated with chromosomal pathology or cardiac ducts in 90% of cases. But in 5% of cases, false positive results are also possible, when a reversal is detected, but everything is fine with the child.
Let us repeat once again that the study did not include all pregnant women, but only those with high genetic risks. This is age over 35 years, a history of the birth of children with hereditary pathologies, stillbirths, increased thickness of the nuchal translucency, etc.
Diagnostic errors
In addition to the fact that the venous duct has a small diameter, the image from it also changes from the movements of the fetus and from the movements of the woman’s anterior abdominal wall. Therefore, research should be trusted only to professionals!
In addition, the hepatic vein passing nearby may also be superimposed on the Dopplerogram of the ductus venosus. Even normally, the presence of reverse is allowed in it, and when layered, it is transferred to the vessel under study, which can be mistakenly taken for reverse in the fetal venous duct.
What to do if reverse blood flow is detected in the ductus venosus in the fetus?
Provided that ultrasound with Doppler sonography is done correctly and there are no artifacts, reverse blood flow in the venous duct should be treated as follows:
- if a woman is not included in a high-risk group, then within a week a detailed ultrasound examination of the fetal heart is performed and a genetic consultation is indicated;
- If, simultaneously with the reverse, a decrease in the nasal bones and a thickening of the nuchal space are revealed, then karyotyping is indispensable. To do this, either amniocentesis or chorionic villus biopsy is performed.
It turns out that reverse blood flow in the ductus venosus in the fetus is just an argument for more detailed and targeted diagnostics during pregnancy.
Ksk in the ductus venosus
The ductus venosus (DV) is a narrow tube-shaped vein with an isthmic entrance, which is a direct communication between the umbilical vein and the central venous system, through which a flow of well-oxygenated blood is formed, bypassing the hepatic circulation. The diameter of the VP is 3 times smaller than the diameter of the intra-abdominal part of the umbilical vein, and its length is only 2-3 mm outside of pregnancy. Due to the presence of a smooth muscle sphincter innervated by fibers of the solar plexus, the phrenic nerve and the vagus nerve, the VP plays an active role in regulating the volume of arterial blood flowing through it. In a normally developing pregnancy, throughout all phases of the fetal cardiac cycle, blood flow in the VP remains unidirectional, representing a three-phase curve. In one cardiac cycle, ventricular systole, early diastole, reflecting passive filling of the ventricles, and late diastole, active contraction of the atria, are distinguished.
Despite the small size of the ductus venosus, the assessment of CSC in this vessel is possible in most fetuses outside of pregnancy. Such high results were obtained primarily by experts, since when obtaining the spectrum of blood flow in the VP, its “contamination” from neighboring vessels often occurs. In addition, “contamination” with signals from the middle hepatic vein can cause false reverse values of blood flow in the VP during the phase of atrial contraction. The movement of the mother's abdominal wall and the behavioral reactions of the fetus itself cause a displacement of the VP during the recording of the SSC. Therefore, optimal registration and interpretation of CSCs in EP obtained in the first trimester of pregnancy is only possible for a very experienced and conscientious specialist working with high-quality ultrasound equipment.
However, it should be noted that in the hands of an expert, the study of blood flow in the venous duct at the end of the first trimester of pregnancy is possible using middle-class devices even without the color flow mode.
Considering the insufficiently high reproducibility of assessing blood flow indices in the VP, most specialists use zero and reverse values of blood flow during the phase of atrial contraction as diagnostic criteria for pathological CSCs. According to most researchers, assessment of blood flow in the VP in early pregnancy should be carried out in patients at high risk of having a child with SCA and congenital defects.
For the first time, these changes in the blood flow in the fetal venous duct with a chromosomal defect were described by T. Huisman and S. Bilardo in 1997. Reverse blood flow in the VP during the phase of atrial contraction and an expanded nuchal space of up to 8 mm were found in one fetus with trisomy 18 from twins in 13 weeks of pregnancy.
In our country, for the first time, the reverse values of blood flow during the phase of atrial contraction in fetuses with CA were reported by M.V. Medvedev et al. and I.Yu. Kogan et al. in 1999. In the observation of I.Yu. Kogan et al., reverse values of blood flow in the VP during the phase of atrial contraction were found at 12 weeks of pregnancy in a fetus with trisomy 21. In the case we described, similar changes in blood flow in the VP were detected in a fetus with trisomy 18 outside pregnancy. The table presents summary literature data on the frequency of occurrence of zero and reverse values of blood flow in the VP during the phase of atrial contraction during fetal CA. The data presented indicate a fairly large scatter in the frequency of pathological CSCs in the venous duct in CA - from 58 to 100%. These results can apparently be explained by the following reasons.
Firstly, zero and reverse values of blood flow in the VP during the phase of atrial contraction are a marker of fetal CAU only at certain stages of pregnancy. Thus, according to E. Antolin et al., the pathological spectrum of blood flow in the EP in CA is significantly more common at gestational age (76.9%) compared to the first week of pregnancy, when abnormal blood flow velocity curves were recorded only in 42.2% of all chromosomal defects. The transient nature of pathological CSCs in the venous duct with an abnormal karyotype of the fetus in early pregnancy is also indicated by A.A. Morozova and E.A. Shevchenko. Considering that the studies were conducted at different times, this fact may have influenced the different frequency of detection of pathological SSCs in the VP of fetuses with CA.
Secondly, it is known that CA is often accompanied by congenital heart defects (CHD), which in early pregnancy can lead to changes in blood flow in the VC. Summary data from different research groups on the incidence of pathological blood flow in the VP during early stages of congenital heart disease are shown in the table.
Thirdly, zero and reverse values of blood flow in the VP during the phase of atrial contraction can also be recorded in fetuses with a normal karyotype. It should be emphasized that in many studies the frequency of false positive results did not exceed the level of 5%, which is accepted as the “gold standard” in prenatal diagnosis. However, with the expansion of the nuchal space in the fetus, both with CA and with a normal karyotype, the frequency of pathological SSCs in the VP increases significantly. In this case, changes in blood flow in the VP are often transient.
In conclusion of this chapter, it should be emphasized that currently the main echographic marker of CA in early pregnancy is the expansion of the fetal nuchal space. In cases where this marker is detected, prenatal karyotyping is a necessary component of prenatal examination in early pregnancy. At the same time, Doppler technologies and assessment of the fetal nasal bones should be considered important additional signs that can improve the efficiency of early prenatal diagnosis of CA, especially in cases of borderline or “controversial” expansion of the nuchal space. It should also be remembered that in some cases, assessment of the fetal nasal bones and detection of pathological SSCs in the VP makes it possible to diagnose CA with normal values of the nuchal space. And in cases where the nuchal translucency is expanded, the additional detection of pathological SSCs in the VP and the absence/hypoplasia of the fetal nasal bones makes it possible to more convincingly explain to patients the need for prenatal karyotyping.
Standards for first screening during pregnancy: what to do if everything is bad?
For some reason, the procedure called “screening” (from English - screening - sifting) causes anxiety in most expectant mothers, some of whom refuse the procedure only because they are afraid to hear unpleasant news about its results.
But screening, especially with the use of modern computer systems and high-precision instruments, is not fortune-telling, but an opportunity to look into the future and find out what the probability is that in due time a baby will be born with an incurable disease.
For parents, this is an opportunity to decide in advance whether they are ready to take care of a child who will require enormous attention and care.
Norms for first screening during pregnancy
First trimester screening essentially consists of two procedures already familiar to women: ultrasound and blood sampling.
When preparing for procedures, it is important to follow your doctor's recommendations and try to remain calm.
Ultrasound standards
During an ultrasound examination, a specialist examines in detail the structure of the embryo, and specifies the gestational age based on indicators such as the coccygeal-parietal size of the embryo (CTE) and the biparietal size of the fetal head (BF).
And, most importantly, it takes the necessary measurements that are informative for assessing the condition of the fetus.
This is, first of all:
- Nuchal translucency thickness (NTT) is the most important indicator during ultrasound to identify the risk of chromosomal pathologies.
Norms for TVP depending on the age of the embryo
If TVP exceeds the normal value, then this is a reason to suspect the presence of a chromosomal abnormality in the fetus.
- Determination of the nasal bone - it is visualized already at 10 - 11 weeks of pregnancy, and at the 12th week it should be at least 3 mm. This is true for 98% of healthy embryos.
- Fetal heart rate (HR) - depending on the week of pregnancy, the following are considered normal indicators:
An increased heart rate in the fetus is also one of the signs of Down syndrome.
- Spectrum of blood flow in the ductus arantius (venous) in the fetus. A reverse blood flow waveform occurs in only 5% of embryos without chromosomal abnormalities.
- The size of the maxillary bone of the fetus - its lag in size is typical for embryos with trisomy.
- Bladder volume – at the age of 12 weeks, the bladder is determined in most healthy embryos only from the 11th week. An enlarged bladder is an additional possible sign of Down syndrome in the fetus.
Biochemical blood test standards
If possible, you should donate blood for a screening examination on the day of the genetic ultrasound or, if this is not possible, the very next day.
Ideally, blood for a screening test is taken in the morning on an empty stomach, or, in extreme cases, no less than 4 hours after a meal.
In the first trimester, screening to identify the degree of risk for the presence of embryonic malformations consists of assessing two indicators: the free β-subunit of hCG and PAPP-A.
The “range” of the values of these blood markers acceptable at each stage of pregnancy (by week) is quite wide and may vary in screening loci depending on the ethnic composition of the region.
However, in relation to the median of a given region - the average normal value for a specific stage of pregnancy - the level of the analyzed indicators should be from 0.5 to 2 MoM.
Moreover, when calculating the risks in each individual case, it is not the pure MoM that is taken, but the one calculated adjusted for the anamnesis of the expectant mother, the so-called. adjusted MoM.
Free β-subunit of hCG
When assessing the risk of developing chromosomal diseases of the fetus, the analysis of free β-hCG is more informative than the level of the hCG hormone itself.
Because The cause of changes in hCG in a woman may be conditions not related to bearing a baby (hormonal diseases, taking certain medications, etc.).
Whereas the predictable change in the level of the β-subunit of hCG is specific to the state of pregnancy.
With a normally developing embryo, the levels of free β-hCG in a woman’s blood will be approximately as follows:
Provided that the gestational age is established correctly and, neglecting the possibility of a false result, the reasons for the discrepancy between the level of β-hCG in a woman’s blood and the gestational age may be completely different reasons not related to abnormalities in the development of the fetus.
RAPP-A standards
A pregnancy-specific protein is produced by the outer layer of the placenta and is observed in the woman’s blood throughout pregnancy.
Its level increases according to the duration of pregnancy.
Limits of PAPP-A indicators in the blood of a patient during a normally developing pregnancy
The value of PAPP-A, as a marker of chromosomal pathologies of the fetus, is alarming when the value is lower than the average in the region (MoM below 0.5). In the first trimester, this may mean a risk of developing Down and Edwards syndromes.
It must be borne in mind that after the 14th week of pregnancy, to determine the risk of developing Down syndrome in the fetus, the PAPP-A level is not informative, because compared with those of a healthy pregnancy, even in the presence of trisomy 21.
Decoding the results of the first screening
To evaluate the results of prenatal screening tests, certified computer programs are used, developed specifically for these purposes and configured to work in the home laboratory.
Therefore, all studies must be completed at one institution.
Only combined screening - assessment of ultrasound data in conjunction with the analysis of biochemical blood markers - becomes the key to obtaining a highly accurate prognosis.
The indicators of a double biochemical test performed in the first trimester of pregnancy are considered in combination with each other.
Thus, a low level of PAPP-A in combination with an increased level of β-hCG in a woman’s blood, all other things being equal, gives serious grounds to suspect the development of Down syndrome in the fetus, and in combination with a reduced level of β-hCG - the risk of developing Edwards syndrome.
In this case, the data from the ultrasound protocol become decisive for making a decision about sending a woman for invasive diagnostics.
If the ultrasound does not reveal any pathological abnormalities in the fetus, then, as a rule, the expectant mother is recommended to undergo repeated biochemical screening, if the duration of pregnancy allows, or to wait for the opportunity to undergo screening in the second trimester.
Unfavorable results of the first screening
Screening data is processed by a “smart” computer program, which issues a verdict on the level of risk for the development of chromosomal pathologies in the fetus: low, threshold or high.
In our country, a risk value of less than 1:100 is considered high. This means that one in a hundred women with similar results of the first screening will give birth to a child with developmental defects.
And such a risk is a clear indication for an invasive examination method in order to diagnose chromosomal diseases of the embryo with 99.9% confidence.
Threshold risk means that the risk of having a child with incurable developmental disabilities ranges from 1:350 to 1:100 cases.
In this situation, the woman requires consultation with a geneticist, whose task, after an individual appointment, is to determine whether the expectant mother is in a high or low risk group for carrying a fetus with developmental defects.
As a rule, the geneticist suggests that the woman calm down, wait and undergo additional non-invasive examinations in the second trimester (second screening), after which she invites her to a second appointment to review the results of the second screening and determine the need for invasive procedures.
Fortunately, the lucky women whose first trimester screening shows a low risk of carrying a sick child: more than 1:350, the vast majority among expectant mothers. They do not require additional examinations.
What to do if you have unfavorable results
If, based on the results of prenatal screening, the expectant mother is found to have a high risk of having a child with congenital malformations, then her first priority is to maintain peace of mind and plan her further actions.
Future parents should determine how important it is for them to have accurate information about the presence of pathologies in the development of the unborn child, and in this regard, decide whether to continue examinations to make an accurate diagnosis.
What to do if you receive poor results after the first screening?
- The first screening should not be repeated in another laboratory.
This way you will only waste precious time. And even more so, you shouldn’t wait for the second screening.
- If you receive poor results (if the risk is 1:100 or lower), you should immediately seek advice from a geneticist.
- You should not wait for a scheduled appointment at the LC and seek a referral or appointment with a geneticist.
You need to immediately find a qualified specialist and attend a paid appointment. The fact is that the geneticist will most likely prescribe an invasive procedure for you. If the period is still short (up to 13 weeks), then this will be a chorionic villus biopsy.
- All women with a high risk of having a child with genetic abnormalities are better off undergoing a chorionic villus biopsy, since other procedures to identify the genotype of the fetus, amniocentesis and cordocentesis, are carried out at a later date.
Results from any invasive procedure should take approximately 3 weeks. If you do the analysis for a fee, then a little less.
- If fetal developmental anomalies are confirmed, then, depending on the family’s decision, the doctor may issue a referral to terminate the pregnancy.
In this case, termination of pregnancy will be carried out within a week.
Now imagine if you do amniocentesis in a week. Wait another 3 weeks for results. And at 20 weeks you are offered to terminate the pregnancy, when the fetus is already actively moving, when there is full awareness that a new life is living in your body.
After 20 weeks, a viable baby can be born in a good clinic. For periods over 20 weeks, abortions are not performed, but artificial births are performed for medical reasons.
Such interventions break the psyche of the woman and the father of the child. It's very hard. Therefore, it is at 12 weeks that a difficult decision should be made - to find out the truth and have an abortion as early as possible. Or accept the birth of a special child as a given.
Reliability of screenings and the need for them
From expectant mothers in queues to see a doctor in antenatal clinics, on thematic forums, and sometimes from doctors themselves, you can hear very different opinions about the advisability of screening during pregnancy.
And indeed. Screenings are not very informative. They do not provide a definitive answer to the question of whether your child has a genetic disorder. Screening provides only a probability and also creates a risk group.
The first screening gives parents the opportunity to conduct a more accurate diagnosis and terminate a short pregnancy or prepare as much as possible for the birth of a special child.
The absence of risks for the development of abnormalities in the development of the fetus, due to chromosomal pathologies, according to screening will allow a young mother to calmly carry her pregnancy to term, being 99% sure that her baby is out of trouble (since the likelihood of false positive results from screening is negligible).
Disputes about the need to undergo screenings and their moral side, apparently, will not subside soon. However, when answering the question of whether it is worth accepting a doctor’s referral for screening, future parents should mentally move forward a few months and imagine a situation where the risks were justified.
And only after realizing their readiness to accept a special baby can mom and dad confidently write a waiver or agree to examinations.
117 COMMENTS
Help me figure out the fetal heart rate is 154 beats/min. KTR 75.0mm. TVP 2.10mm. Free beta subunit of hCG 21.70 IU/l /0.673MoM. PAPP-A 13.190 IU/l / 2.648 MoM. Trisomy 21 base risk 1: 126. Individual risk 1: 2524. Trisomy 18. basic risk 1:324 individual risk 1:6483. Trisomy 13 base risk 1:1012.<1:20000
Based on the data you provided, we can draw the following conclusions.
- An ultrasound examination in the 1st trimester of pregnancy is carried out to determine the risk of Down syndrome in the fetus. It is carried out from 10 weeks 6 days to 13 weeks 6 days of gestation. Earlier or later research is ineffective.
- The fetal heart rate depends on the stage of pregnancy and is 161–179 beats per minute in the 10th week of pregnancy, 150–174 beats per minute in the 12th week of pregnancy.
- The CTE of the fetus for effective ultrasound should be more than 45 mm.
- TVP is normally in the range of 1.5–2.2 mm at the 10th week of gestation, 1.6–2.5 at the 12th week.
- The results of biochemical screening indicate an increased risk of having a child with Down syndrome and Edwards syndrome.
- Normally, the free beta subunit of hCG is from 0.5 to 2.0 MoM, and PAPP-A is from 0.5 to 2.5 MoM. IU/l data depends on the laboratory and its interpretation is given separately.
- Risks for deviations from the norm must be more than 1:380. You are at increased risk for trisomy 21, or Down syndrome, and trisomy 18, or Edwards syndrome.
To obtain reliable information, you need to contact a antenatal clinic with the results of the research. Based on all the data obtained, you will be offered appropriate pregnancy monitoring.
If necessary, you will be asked to undergo an invasive diagnostic method in the form of amniocentesis to determine possible pathologies in the fetus.
Please help me understand the results of an ultrasound examination in the 1st trimester (13-14 weeks) heart rate 158 per minute. KTR 76.0 mm. TVP 1.37mm. BPR 26.8 mm. Exhaust gas 95.0 mm. Coolant 77.0 mm. DlB 14.0 mm. Risk with Down syndrome is low 1:1501
You do not indicate the exact gestational age based on ultrasound. Does it coincide with the date of the last menstruation?
Another important indicator during an ultrasound examination in the 1st trimester of gestation is the visualization and thickness of the nasal bone. This indicator is one of the markers for the risk of a fetus having Down syndrome.
Ultrasound screening in the 1st trimester of pregnancy is performed from 10 weeks 6 days to 13 weeks 6 days. An earlier or later study is not informative.
With an ultrasound examination in the 1st trimester, the doctor determines the size of the fetus, gestational age, location and condition of the placenta, and the risk of Down syndrome in the child.
Based on the data you provided, we can draw the following conclusions.
- The fetal heart rate at the 13th week of gestation is in the range of 147–171 beats per minute.
- The average CTE is 63–74 mm at the 13th week, and 63–89 mm at the 14th week.
- The normal TVP is 0.7–2.7 mm. An increase in the thickness of the nuchal translucency is evidence of an increased risk of having a child with Down syndrome.
- BPR at the 13th week is in the range of 20–28 mm, at the 14th week – 23–31 mm.
- OG at the 13th week is 73–96 mm, at the 14th week – 84–110 mm.
- Coolant at the 13th week varies between 58–80 mm, at the 14th week – 66–90 mm.
- Dlb at the 13th week is normally 7.0–11.8 mm, at the 14th week – 9.0–15.8 mm.
The risk for Down syndrome is calculated by a special computer program that takes into account the data obtained during an ultrasound examination, the woman’s age, a burdened medical history with the presence of children with Down syndrome in the woman or her close relatives, including her husband’s side. Normally, this figure should be 1:380 or less.
According to the data you provided, you are not in the risk group for having a child with Down syndrome.
To obtain reliable information, you need to contact an obstetrician-gynecologist with the results of the 1st screening ultrasound.
Thanks a lot! At least a little, but they calmed me down) they’ll look more accurately at the second ultrasound)
Good afternoon, help me understand the adjusted Mom and calculated risks
fb-hCG 92.6 ng/ml 3.50 Accor MoM,
PAPP-A 10.5 mlU/ml 2.37 Accor MoM,
Corrected MoM and calculated risks when conducting biochemical screening during pregnancy are necessary to obtain the risks of having a child with a congenital pathology.
MoM is the coefficient of the degree of deviation from the average normal values. Is universal for all laboratories.
The MoM may deviate depending on a number of factors:
The race of the woman;
Bad habits, including smoking;
Number of fetuses in the uterus;
Concomitant diseases, including diabetes, hypertension;
Pregnancy through IVF.
Adjusted values of indicators are calculated adjusted for risk factors. As a result, the absolute and adjusted MoM values may differ significantly.
The normal values for fb-hCG in ng/ml and PAPP-A in mlU/ml are different for each laboratory. When issuing test results, there is a column with standards for a given laboratory.
The norm for MoM ranges from 0.5 to 2.0 MoM.
In your case, there is not enough data to decrypt.
If we take into account only the MoM provided by you, we can note an increase in both indicators relative to the norm. This may be due not only to an increased risk of having a child with a congenital anomaly, but also to the characteristics of pregnancy or the development of two or more fetuses.
To receive a full transcript, you need to provide the research findings to your obstetrician-gynecologist. If necessary, you will be referred for an invasive test, or amniocentesis, to obtain reliable information.
Hello, help me understand the results of the 1st ultrasound screening. Pregnancy period: 12 weeks, 6 days body length - 63, femur length - 8.6, nasal bones - two 2.2 mm each, without any features.
For your conclusion, you did not indicate the main indicator - the risk of developing Down syndrome, which is determined based on the results of an ultrasound study, the woman’s age and the presence of risk factors for the development of the pathology.
Your data indicates the following:
CTE at 12 weeks 6 days of gestation is 51–73 mm.
Heart rate at 12–13 weeks is in the range of 150–174 beats per minute.
TVP from the 12th week to 12 weeks 6 days is in the range of 0.7–2.5 mm. The average value is 1.6 mm. An increased risk is established when the TVP increases above 2.5 mm.
BDP from the 12th to 13th week of gestation is 18–24 mm.
Normal exhaust gas is 58–84 mm.
Coolant normally varies from 50 to 72 mm.
Dlb at the 12th week of pregnancy is 4.0–10.8 mm.
The nasal bones should be visualized and range from 1.8 to 2.3 mm.
Blood flow in the ductus venosus should not normally be zero or reverse.
The ultrasound screening data you provided for the 1st trimester of pregnancy is within normal limits.
To confirm the normal course of pregnancy and the absence of risk of having a child with Down syndrome, you need to consult a gynecologist at the antenatal clinic at your place of residence. You must have an ultrasound doctor's report with you.
Good afternoon, I need your help. The Uzist almost gave me a heart attack. She was very rude. And as soon as she began to move it over her stomach, she rudely shouted: You have an anomaly. You need to see a geneticist. She didn’t explain anything, she just was rude and tried to understand that this screening was a death sentence! Here's the conclusion:
The thickness of the collar space is 4.3 mm; the nasal bones are visualized to be 1.0 mm long; pulsation index in the ductus venosus 1.07/reverse. The coccygeal-parietal size of the embryo is 54 mm. The purity of the heartbeat is 159 beats per minute. Pregnancy 12.1 weeks.
The conclusion you described lacks data. To complete the picture, you need to know your age and the presence of risk factors for having a child with Down syndrome, as well as the full conclusion of the ultrasound screening.
In ultrasound screening, which is performed from 10 weeks 6 days to 13 weeks 6 days of pregnancy, the main thing is the conclusion about the risk of Down syndrome. This parameter is calculated automatically by a computer program.
In addition, ultrasound examination should indicate the dimensions of the head in the form of biparietal size and circumference, abdominal circumference and thigh length. Another important indicator is the location and condition of the placenta, through which the child receives the necessary nutrients for normal growth and development.
Based on the data you provide, the following conclusions can be drawn.
- KTP, or coccygeal-parietal size at 12–13 weeks of gestation is 51–59 mm.
- The fetal heart rate should be between 150 and 174 beats per minute.
However, you should not rely only on ultrasound data. In order to confirm or refute pathology in the fetus, you need to immediately contact a gynecologist at the antenatal clinic.
Based on all the data received from you, the specialist will prescribe further examination, which includes non-invasive and invasive procedures.
Non-invasive interventions include biochemical screening with determination of beta-hCG and PAPPA-A levels. The study allows you to calculate the risk of a chromosomal abnormality in the fetus.
Based on the results of studies, if there is an increased risk of having a child with a congenital pathology, you will be offered to undergo invasive intervention in the form of amniocentesis, cordocentesis or chorionic villus biopsy.
And remember that stress and anxiety in your position are unacceptable.
Hello! I had a screening done at 12 weeks and 6 days, KTR 64, TVP 1.7 mm, elevated hCG 2.578, other indicators were normal. Risk 1:687. Please tell me something is wrong? What is the likelihood of developing pathologies in a child?
There is not enough data to reliably assess the result. To complete the picture you need to know:
- Your age.
- Do you or your immediate relatives have children with Down syndrome or other genetic pathologies?
- A complete picture of the ultrasound screening, indicating the dimensions of the head, abdomen, femur length, visualization and thickness of the nasal bone. The nasal bone becomes accessible from 11 weeks of gestation.
- Risks due to a genetic abnormality after a biochemical study.
- You indicate the risk of 1:687, but do not specify what kind of screening it is: ultrasound or biochemical.
The risk of a chromosomal abnormality should normally be more than 1:380 based on the results of ultrasound and biochemical screening.
The CTE of the fetus at 12 weeks of gestation ranges from 51 to 59 mm, at 13 weeks - from 62 to 73 mm.
TVP at 12 weeks is in the range of 1.6–2.5 mm. An increased risk of having a child with Down syndrome is established when this indicator exceeds 3 mm.
The data you indicated from the ultrasound screening are within normal limits.
Normally, the free beta subunit of hCG is in the range of 0.5–2.0 MoM. In your case the indicator has been increased.
Elevated hCG levels may be associated with:
- Down syndrome in the fetus;
- multiple pregnancy with two or more fetuses;
- toxicosis of the first half of pregnancy;
- the presence of concomitant diseases in the mother, including diabetes mellitus, arterial hypertension.
In order to obtain reliable information, you should contact your attending obstetrician-gynecologist, who, based on all the data, will make a conclusion and develop tactics for further pregnancy management, adjusted for concomitant diseases. If indicated, you will be offered to undergo a second biochemical screening or invasive intervention in the form of amniocentesis.
Based on the risk you indicated, I can say that 1 woman out of 687 can give birth to a child with a congenital pathology. This indicator belongs to the low-risk group.
I am 25 years old, I have no relatives with any pathologies either on my husband’s side or on mine. Ultrasound at 12.3 weeks ktr 64 mm, heart rate 160, tvp 1.7 mm, nasal bone 1.5 mm. Chorionic presentation. They did an ultrasound and immediately took blood from a vein.
Hello, please help me figure it out. They suggest doing a puncture because there are risks. Screening 12 days and 4 days.
Weight: 56.1 Height: 153 Age: 33.
Intracranial space 2.2mm
Ductus venosus 0.90
Nasal bones 2.4 mm
Free hCG beta subunit 6.70 IU/l equivalent to 0.184 MoM
PAPP-A 0.628 IU/l is equivalent to 0.187 MoM
Trisomy 21: basic (1:407) individual (1:8144)
Trisomy 18: basic (1:995) individual (1:335)
Trisomy 13: basic (1:3121) individual (1:22)
Have you or your close relatives had pregnancies with an established genetic pathology?
Let's look at the results of your screening. Let's start with ultrasound research.
You do not indicate what the risk for Down syndrome was according to the ultrasound. In addition, for correct interpretation of the data, it is necessary to indicate all fetal dimensions: BPD, head circumference and femur length. The condition of the placenta is of no small importance.
- The fetal heart rate at 12–13 weeks of pregnancy should be 150–174 beats per minute.
- CTE at 12–13 weeks of gestation is in the range of 51–73 mm. At 12 weeks 4 days, CTE can be from 49 to 69 mm.
- TVP normally varies from 1.6 to 2.5 mm.
- The intracranial space should be between 1.5 and 2.5 mm.
- The ductus venosus should not have negative values and not have reverse.
- The nasal bones begin to be visualized from the 11th week of pregnancy. Their normal thickness is 1.8–2.3 mm.
Based on the data you provided, we can conclude:
- The fetus experiences a slight increase in heart rate, which may indicate hypoxia. It is necessary to know the condition of the placenta.
- If tachycardia is associated with insufficient functioning of the placenta, hospitalization in the gynecological department is necessary.
- Lack of oxygen for the fetus may be associated with bad habits of the mother, among which smoking is the most harmful.
Let's look at biochemical screening.
- Normally, the free beta-hCG subunit and PAPP-A range from 0.5 to 2.0 MoM.
- Your biochemical screening data is within normal limits. The exception is the individual risk of trisomy 13, or Patau syndrome.
The risk of having a child with trisomy 13 is 1 in 22 women. This indicator belongs to the high-risk group. Perhaps you or your close relatives previously had children with developmental anomalies, which led to such indicators.
To make sure that the baby is healthy, you should undergo an invasive procedure in the form of amniocentesis followed by genetic counseling.
Irina Vyacheslavovna thank you very much.
Age 43
Among the relatives there is no one with pathologies; there is a 15-year-old child who is healthy.
Two STs in 2014 and 2015.
Term 12n6d according to m, 12n3d according to ultrasound
Fetal CTE 59.7, BPR 21.1, TG 75.8, OB 65.7, DB 8.2, HR 162, no defects in the calvarial bones, TVP 2.5, nasal bones 1.8, normal blood flow, anterior chorion localization, fetal weight 65+/-9
Risks due to a genetic abnormality after a biochemical blood test:
PAPP-A 0.422, fb-hCG 2.39
age risk 1:30
Biochemical risk T21 1:50
Combined risk for Trisomy 21 1:50
Trisomy 13/18 +TE 1:50
MoM of the neck fold 1.61
Currently the term is 13.5 according to ultrasound
The age-related risk of having a child with Down syndrome increases after a woman reaches 40 years of age.
Due to the fact that you are 43 years old and have a history of 2 missed pregnancies, you will be asked to undergo an invasive procedure in the form of amniocentesis. In addition, you have increased risks based on the results of the first screenings.
Let's analyze all the data.
The gestational age according to ultrasound and menstruation can vary within 7 days, which depends on the time of ovulation and fertilization of the egg.
- The normal CTE of the fetus at 12–13 weeks of pregnancy is 51–73 mm.
- The fetal BPD is 18–24 mm.
- Exhaust gas - 58–84 mm.
- Coolant - 50–72 mm.
- DB - 4.0–10.8 mm.
- The fetal heart rate should vary between 150–174 beats per minute.
- TVP should normally be 1.6–2.5 mm.
- The nasal bones should be visualized and their thickness should be between 1.8 and 2.3 mm.
You do not indicate what the risk for Down syndrome is based on the results of ultrasound screening. This indicator is calculated automatically by a special program.
All the data you provided is within normal limits. However, the thickness of the nasal bones and TVP are at the lower limits of normal, which, together with age, will make the risk result higher.
According to the results of a biochemical study, PAPP-A and fb-hCG should be from 0.5 to 2.0 MoM.
You have an increase in the free beta-hCG subunit, which may be associated with the presence of Down syndrome in the fetus or result from concomitant pathology.
Risks after studies should be more than 1:380. Your risks are increased. This means that with tests like yours, 1 woman in 50 has a chance of giving birth to a child with a genetic pathology.
To clarify the diagnosis, you need to immediately contact your treating gynecologist, who, based on all the data, will be able to develop tactics for further pregnancy management.
You will be asked to undergo amniocentesis to make a correct diagnosis.
Pregnancy period: 12 weeks 3 days, ktr 57mm, hCG 41.5 ng’ml, rrr-a 1365.6ml, tvp 0.1mm
Down syndrome.v.risk.1:1417 estimated risk. 1:5712
Sind.Edwards. age.risk.1:1274 calculated risk. 1:1000
Hello, I'm Lisa. Help me find out. Thank you. Can not wait.
To obtain accurate information, you need to contact the gynecologist at your place of residence with the results of the study.
You are providing insufficient information. For an accurate conclusion, it is necessary to know all the parameters based on the results of ultrasound and biochemical screening. For reliability it is necessary:
- Anamnestic data indicating whether you or close relatives have a genetic pathology.
- Fetal dimensions: head size, abdominal circumference, thigh length.
- Fetal heart rate.
- Visualization of the nasal bone and its thickness.
- Condition of the placenta.
- Biochemical test data in MoM, or international units, which are the same for all laboratories.
- If you indicate data in ng/ml, then you must indicate the standards of the laboratory where you donated blood for testing, since the data may differ.
- Normal CTE at 12–13 weeks of pregnancy is in the range of 51–73 mm.
- The normal TVP is 0.7–2.5 mm.
- After biochemical screening, the risks should be more than 1:380.
Based on the risks you indicated, you do not fall into a group at high risk of having a child with a genetic abnormality. But only your obstetrician-gynecologist can make a conclusion about a normal pregnancy.
Good afternoon, please tell me. Ultrasound: Term 13.3. KTR -68mm, HR-164, TVP 1.5mm, nose 2.5mm, PI0.25.
Blood: PAPP-A 8.075 IU/l-1.705 Mohm b-hCG 80.86 IU/l - 2.123 Mohm
Help me decipher, the doctor didn’t say anything
Unfortunately, there is not enough data. The full list can be found on the page http://in-waiting.ru/ask-qa (Category “Pregnancy Development”)
Irina Vyacheslavovna, thank you very much for the detailed information, I live in Italy, and it was very difficult to understand the results, there is still a week before my appointment with the doctor, I would be very grateful if you give a brief explanation, Here are my results (I donated blood a week before the ultrasound - the doctor said so):
Date of the first day of the last menstruation 02/28/17
My age is 28; Height 167, weight 53
Duration 12 weeks and 2 days
Baby's heart rate: 156bpm
Top cross length (CRL): 62.0 mm
Diameter biparietal (DVP): 19.0 mm
hcg:57.8 UI equivalent to 1.135 MoM
PaPP-A: 0.904 UI equivalent to 0.355 MoM
Risks of trisomy 21:
basic 1:771 correct 1:630
Risks of trisomy 18:
Base 1:866 correct 1:13014
Risks of trisomy 13:
Basic 1:5858 correct< 1:20000
Does the pregnancy period match according to menstruation and ultrasound?
At this point, if the dates match, you should be 13-14 weeks pregnant. If they do not match, you need to rely on ultrasound screening.
Based on the research results provided by you, the following conclusions can be drawn.
The fetal heart rate at 12–13 weeks of gestation is in the range of 150–174 beats per minute. Your baby's heart rate is within the normal range of 156 beats per minute.
CRL, or CTR, or coccygeal-parietal size at 12–13 weeks varies from 42 to 73 mm. The CTE of your fetus is 62 mm, which is normal.
NT, or TVP, or nuchal translucency thickness is normally in the range of 0.7–2.5 mm and should not exceed 3 mm.
In order to make a conclusion about the result of ultrasound screening, you need to know all the fetal measurements and the risk for Down syndrome, which is calculated automatically.
Biochemical screening results: free beta-hCG subunit and PAPPA-A should be in the range of 0.5–2.0 MoM, and the risks for chromosomal abnormalities should be higher than 1:380.
In your case, neither the baseline nor the adjusted risk values place you at risk for a chromosomal abnormality.
In order to find out accurate information, contact your local gynecologist.
Irina Vyacheslavovna, thank you very much, I am sincerely grateful.
Please help me understand the analyses.
Second pregnancy. Mother's age is 22 years. Weight 52.0kg
Pregnancy 12 weeks + 3 days according to KTR
Fetal heart rate 152 beats/min
Nasal bone: determined; Tricuspid valve Doppler: normal; Doppler measurement of the venous duct: normal;
Free hCG beta subunit: 23.80 IU/l equivalent to 0.580 MoM
RARRA-A: 4.014 IU/L equivalent to 1.378 MoM
Baseline risk: trisomy 21; 1:1035; trisomy 18; 1: 2470; trisomy 13; 1:7763
Individual risk: trisomy 21; 1:20709; trisomy 18; 1:49391; trisomy 13: 1:155262.
The data is not complete enough:
- When was your last period?
- Do gestational dates match according to menstruation and ultrasound?
- How was your previous pregnancy?
- What is the meaning of TVP, or NT, or collar space thickness?
- Dimensions of the fetal head, abdominal circumference and length of the femur?
- What is the risk for Down syndrome based on screening results?
Based on the data provided, the following conclusions can be drawn.
CTE in pregnancy 12–13 weeks is in the range of 51–59 mm.
The fetal heart rate should vary from 150 to 174 beats per minute.
The nasal bone after 11 weeks of pregnancy should be clearly visible and be more than 3 mm.
The ductus venosus normally does not have negative values or reverse.
According to the results of biochemical screening, the free beta-hCG subunit and PAPAA-A should be in the range from 0.5 to 2.0 MoM.
The risks for a chromosomal abnormality, both according to ultrasound screening and biochemical testing, should be greater than 1:380.
The research data you provide is within normal limits. However, there is insufficient data to draw a conclusion.
You need to contact a gynecologist at your place of residence and provide him with all the findings. By comparing anamnestic data, ultrasound and biochemical screening, the doctor will be able to answer what risks you have for having a child with a chromosomal abnormality.
Hello. Please tell me the results of screening for a period of 11 weeks and 4 days.
PAPP-A 0.28 (according to the Life Cyclt program)
Down syndrome 1:475
Edwards Syndrome-(T18)- 1:5862.
I’ll be donating blood to geneticists in a week. Well, now I can’t find a place for myself. Help me understand these indicators.
Please help me understand the analysis
Age 38 years. Weight 110kg
Pregnancy 11 weeks + 3 days
TVP - 1.80 mm (1.40 MoM)
Fetal heart rate 134 beats/min
Nasal bone: determined, 2.3mm;
hCG: 39.2 ng/ml; 0.94 MoM
RARRA-A: 1.04 mlU/ml; 0.95 MoM
Biochemical risk+NT 1:873 (below cut-off), Double test 1:800 (below cut-off), Age risk 1:126, trisomy 13/18<1:10000;
There is not enough data to answer the question of how your child is developing. It is not possible to judge the condition of the fetus only by the results of the study indicated by you.
For a complete picture, you need to contact a gynecologist at your place of residence for tests.
To give an opinion about the child’s condition and the risk of developing a chromosomal abnormality, you need to know:
- History of a woman.
- Full description of ultrasound screening results.
- Conclusion of an ultrasound study indicating the risk of having a child with Down syndrome.
Normally, the risk of a chromosomal abnormality should be higher than 1:380, both according to the results of ultrasound and after a biochemical study.
Every woman over 35 years of age is at increased risk of having a child with Down syndrome. You need to consult a geneticist and, if necessary, conduct additional tests in the form of invasive intervention: amniocentesis, cordocentesis or chorionic villus biopsy.
- Free beta-hCG subunit and PAPPA-A should be between 0.5 and 2.0 MoM.
- At 11 weeks, 3 days of pregnancy, the fetal calf size is 37–54 mm.
- TVP is in the range of 0.8–2.2 mm.
- The nasal bones begin to be visualized from the 11th week of gestation, and their thickness should not exceed 3 mm.
- The fetal heart rate is 153–177 beats per minute.
In your case, it is necessary to know the condition of the placenta, since according to the results of an ultrasound examination, the child has bradycardia, or a decrease in heart rate. To improve the condition of the fetus, you need to undergo a course of treatment.
In addition, bradycardia may be one of the signs of impending spontaneous miscarriage.
To maintain and prolong your pregnancy, you need to urgently consult a doctor.
Tell me, is everything okay?
13 weeks pregnant exactly at the time of screening
Ductus venosus PI 1.040
Choriton/Placenta - low on the anterior wall
Umbilical cord - 3 vessels
hCG - 53.7 IU/l equiv. 1,460 Mohm
PPAP-A - 2.271 IU/l equiv. 0.623 MoM
Trisomy 21 1:10326
Trisomy 18<1:20000
Trisomy 13<1:20000
Preeclampsia before 34 weeks of pregnancy 1:640
Preeclampsia before 37 weeks of pregnancy 1:168
Let's look at all the data you provided. Let's start with being within the normal range.
- The fetal heart rate at 13 weeks of gestation can range from 147 to 171 beats per minute.
- The fetal CTE, or coccygeal-parietal size, at 13 weeks of pregnancy is 51–75 mm, the average value is 63 mm.
- TVP, or nuchal translucency thickness, or NT, is one of the main indicators during the first ultrasound screening, since based on this indicator the risk of having a child with Down syndrome is calculated. Normally, TVP is 0.7–2.7 mm.
- The BPD, or biparietal size of the fetal head should be in the range of 20–28 mm, the average value is 24 mm.
The ductus venosus should have positive values. If the indicator is negative or there is a reversal, this increases the risk of a child developing a chromosomal abnormality.
The fetal umbilical cord normally consists of three vessels: 2 arteries and 1 vein, through which oxygen and nutrients necessary for the development of the fetus are supplied.
To make a conclusion about the condition of the fetus, the following data is not enough:
- Fetal dimensions: head circumference, abdominal circumference, thigh length.
- Visualization and thickness of the baby's nasal bones, which are measured after 11 weeks of pregnancy.
- Visualization of the internal organs of the fetus.
- Conclusion of ultrasound screening for Down syndrome, which is normally more than 1:380.
According to the results of the ultrasound, the placenta in your case is located along the anterior wall. The location of the baby's seat may vary depending on the implantation site. Moreover, for a normal pregnancy, the placenta should be located 7 cm or more above the internal os.
According to the ultrasound, your placenta is located low, which means its location is below 7 cm from the internal os. This indicator is monitored at the second ultrasound. Most often, as pregnancy progresses, the placenta rises and takes a normal position. In the case when its elevation is not carried out, we can talk about the low location of the placenta, which requires the close attention of the woman and the doctor.
According to the results of biochemical screening, the normal levels of free beta-hCG subunit and PAPPA-A are 0.5–2.0 MoM.
Risks are normally higher than 1:380.
In your case, the risk of developing late gestosis is increased. This may be due to the course of this pregnancy and previous ones. The risk increases if a woman had gestosis in a previous pregnancy. To do this, you need to know your obstetric-gynecological and somatic history.
To get reliable information, contact your local obstetrician-gynecologist.
Hello! Help with sorting out the tests: 3rd pregnancy. 30 years
ultrasound 1st trimester 05/16/2017 (estimated pregnancy period 10 weeks 4 days)
fetometry: CTE 48 mm. embryo size = 11 weeks. 5 days
nasal bone 2.2 mm.
general screening: from 05/17/2017 (calculated by ultrasound 11 weeks 5 days)
rrr- A=0.53 MOM. HCG-3.12 MOM
Disease Down Syndrome
Age risk 1:810………..Calculated risk 1:184 -High risk
Disease Down Syndrome only in biochemistry
Age risk 1:810………..Calculated risk 1:28 -High risk
The rest of the indicators were low. I had a geneticist and amniocentesis was recommended.
Question...what week is the calculation based on? At 10 and 12 weeks then the tests will be normal, if at 11 weeks then yes there are risks of increased hCG...
Converted MOM to another unit (ng/ml)…using medians
Which week should I take for calculation? if 1 day of last menstruation. 03/03/2017
The gestational age is calculated based on the results of the 1st ultrasound screening. This is due to the fact that the fetus in the period from 10 weeks 6 days to 13 weeks 6 days has the same size, which is calculated using special tables. After the 14th week of gestation, fetal development varies and depends on genetic characteristics.
Calculation of gestational age by ultrasound is calculated on the basis of data on all sizes of the fetus.
The gestational age according to ultrasound and the date of the last menstruation may differ, depending on ovulation. Ovulation may be early, then the gestational age is longer according to ultrasound. With late ovulation, the gestational age will be shorter according to ultrasound. If ovulation occurred in the middle of the menstrual cycle, the gestational age according to ultrasound and the date of the last menstrual period will coincide.
In order to answer your question correctly, the following information is required:
- Fetal dimensions indicated in mm: BDP, abdominal circumference, thigh length.
- Size, location and condition of the placenta.
- Fetal heart rate.
- Conclusion on the risk of having a child with Down syndrome based on ultrasound screening results.
- Your medical history: have you or your close relatives had children with a chromosomal abnormality?
- How did previous pregnancies end?
- The nature of the menstrual cycle: its regularity, how long after the next menstruation begins, how many days menstruation lasts.
Based on the date of your last menstrual period, your pregnancy should be 17–18 weeks. According to ultrasound screening - 18–19 weeks. A difference within 7 days is not a deviation. The gestational age is calculated using ultrasound screening.
- The CTE of the fetus at 11 weeks 5 days of pregnancy is in the range of 39–57 mm, the average value is 48 mm.
- The normal TVP is 0.8–2.2 mm.
- The nasal bone is clearly visualized after 11 weeks, its average thickness is 1.4 mm. After the 12th week of pregnancy, its thickness should be more than 3 mm.
Based on biochemical screening, free beta-hCG subunit and PAPPA-A should be between 0.5 and 2.0 MoM. The calculation in ng/ml is individual for each laboratory, and the standards are indicated separately.
Risks should normally be more than 1:380.
In your case, the level of hCG and the risks of a chromosomal abnormality are increased.
In order to make sure that the fetus does not have a chromosomal pathology, you need to undergo additional examination in the form of amniocentesis followed by consultation with a geneticist.
Tell me if everything is okay, the doctor said there are abnormalities in the tests. What does this mean? I am 29 years old, 9 months ago I gave birth to my first child. I have no relatives with pathology. At the time of the ultrasound, it was 12.5 days per month, according to the ultrasound 12.2 days .KTR - 56mm.HR-160 beats/min.TVP-1.4 mm.Nasal bone-2.1mm.PI-1.1.PAPP-00.861 MOM.v-hCG - 0.291 MOM.
Hello, I was referred to a geneticist for screening tests. Please tell me if I should worry. I’m 28 years old. Ultrasound: 11 weeks, 4 days, ktr-48mm, bg-16.6mm, heart rate-171 beats, tvp-1.5mm .,ksk in the venous duct - 1.00., length of the nasal bones - 1.5 mm., yolk sac - 3.1 mm., screening: hCG - 91.70 me/l/2.131 mm., PAPP-A-0.373 me/ l/0.255mom., trisomy 21-ind: 1:706, base: 1:58., trisomy 18-ind: 1: 1588, base: 1: 4326., trisomy 13-ind: 1: 5017, base: 1 :3055. Thanks in advance!
Based on the results of screening in the first trimester of pregnancy, you are at high risk of having a child with Down syndrome.
To make sure that the fetus does not have a chromosomal abnormality, you need to consult a geneticist. If necessary, the doctor will refer you for additional research in the form of invasive diagnostics. Depending on the stage of pregnancy, you may be offered a chorionic villus sampling, cordocentesis or amniocentesis.
We will analyze the provided data from your research.
At 11–12 weeks of pregnancy, the norms for the first ultrasound screening are:
- CTE - 38–56 mm, the average value for 11 weeks 4 days is 47 mm;
- BRG - 13–21 mm;
- TVP - 0.8–2.4 mm;
- blood flow in the venous duct is positive, has no reverse values;
- nasal bones are clearly visualized, their thickness is on average 1.5 mm;
- yolk sac - more than 2 mm from 6 to 12 weeks of gestation.
The ultrasound values you indicated are within normal limits. To determine the risk of Down syndrome in a child, you need to know:
- all sizes of the fetus;
- condition of the placenta;
- ultrasound conclusion, in which a special program calculates the risk of a chromosomal abnormality.
According to the results of biochemical screening, the free beta-hCG subunit and PAPPA-A should be in the range from 0.5 to 2.0 MoM, and the risks of chromosomal pathologies are higher than 1:380.
With an increase in beta-hCG, the risk of Down syndrome in the fetus increases. This indicator may also increase as a result of other reasons, such as gestosis, diabetes mellitus or other concomitant diseases.
According to your indicators, a child with trisomy 21 pairs of chromosomes, or Down syndrome, can be born to 1 in 58 women, which is a high risk.
Only your doctor can give you more detailed information.
Hello! Now I am one week pregnant, I only just now found out that I have abnormal blood results from the first screening at 12 weeks, papp -0.41 mom, hCG - 0.42 mom! He didn’t tell me anything about this earlier, although they should have referred me to a gyneticist, as I understand it, but alas, the train has already left! Calculated risk T-21 1:6657, T-18 1:2512, T-13 2:, and according to the program astaria T-13 1:1422, help me decipher I’m going crazy for the second day.
According to the ultrasound and the first and second, everything is fine without pathologies! My doctor on vacation will find out why it happened that they didn’t inform me about the low blood levels. The midwife couldn’t tell me if my results were scary.
Normal values for biochemical screening in the first trimester of pregnancy are free beta-hCG subunit and PAPPA-A from 0.5 to 2.0 MoM.
Deviations from normal values can be caused by a number of factors, including fetal development anomalies and unfavorable pregnancy.
A simultaneous decrease in beta-hCG and PAPPA-A levels may occur with an increased risk of developing Edwards syndrome in the fetus. In addition, indicators may be reduced if spontaneous miscarriage threatens.
The estimated risk for a chromosomal abnormality in the fetus should be higher than 1:380 for all indicators.
Your calculated risks are within normal limits.
When detecting reduced levels of beta-hCG and PAPPA-A, the doctor is guided by ultrasound screening data. If the study reveals deviations from the norm, it is necessary to undergo a consultation with a geneticist and, if indicated, conduct additional research in the form of an invasive intervention.
If the ultrasound screening results do not reveal any abnormalities, it is recommended to undergo a second screening test at 16–20 weeks of pregnancy.
To resolve any questions you may have, you need to contact the antenatal clinic at your place of residence.
Good afternoon, please help me decipher this, I am 28 years old, the screening was at 11 weeks. Blood results -PAPP-A-4.33, -cor.mom 1.96, free beta hCG-134, corr.mom 2.63.biochemical risk + NT on the date of sample collection 1:7076 below the cutoff, age-related risk at date of sample collection 1:726, trisomy 13/18+NT<1:10000 ниже пор. Отсечки.помогите расшифровать пожалуйста!
You have undergone biochemical screening in the first trimester of pregnancy, which is carried out from 10 weeks 6 days to 13 weeks 6 days. At the same time, the first ultrasound examination is scheduled.
The assessment of the fetal condition is carried out based on the totality of studies performed: biochemical and ultrasound screenings. If there are deviations, the woman is referred to a geneticist for consultation. If indicated, additional invasive research is performed in the form of cordocentesis, chorionic villus biopsy or amniocentesis, depending on the gestational age.
Normally, the results of biochemical screening indicators for free beta-hCG subunit and PAPPA-A are in the range of 0.5–2.0 MoM.
The estimated risks for the development of a chromosomal abnormality in the fetus should be higher than 1:380 for all indicators.
The corrected MoM value normally varies from 0.5 to 2.0 MoM. This indicator is calculated by a special computer program individually for each pregnant woman. In this case, adjustments are made for age, anamnestic features and a number of other factors.
Based on the biochemical screening indicators provided by you, we can conclude that the child is not at risk for developing a chromosomal abnormality if an error was made in the writing and instead of 134 MoM there should be 1.34 MoM of the free beta-hCG subunit. If this indicator is elevated, this may indicate fetal pathology.
To obtain correct information, I recommend that you contact an obstetrician-gynecologist at your place of residence. After studying the results of biochemical and ultrasound screenings together, the doctor will choose further tactics for managing your pregnancy.
Good afternoon, I’m now in Bulgaria, I had an ultrasound and biochemical screening at 12 weeks and 3 days, the first day of my last period was April 8, before that my cycle was disrupted, the date of conception was April 23, I donated blood on July 14, 2017. I’m 33 years old and weigh 85 kg. , according to the ultrasound, the doctor said that everything was fine, but she didn’t give any conclusions with measurements, only a photo of the baby, I’m very worried about the results of the analysis, I can’t decipher it, please help
Risk of Down syndrome 1 in 12,000
Edwards syndrome 1 in 29,000
Patau syndrome 1 k
Turner syndrome 1 k
Biochemical risk of Down 1 in 4300
Age risk 1:54
Free bCG 0.33 MoM
In order to give an opinion about the condition of the fetus, it is necessary to know the results of ultrasound and biochemical screenings of the first trimester together. These studies allow us to get a complete picture.
Ultrasound allows you to take measurements of the fetus in order to identify pathologies of the child’s organ systems. In the gestation period from 10 weeks 6 days to 13 weeks 6 days, all fetuses have similar parameters; after the 14th week of gestation, the child begins to develop individually, which is genetically determined. In addition, the thickness of the collar space and nasal bones is measured. Based on the data obtained, the risk of Down syndrome in the fetus is determined. The condition of the placenta is important.
Normal free beta-hCG subunit and PAPPA-A range from 0.5 to 2.0 MoM. Risks for chromosomal abnormalities should be above 1:380 for all indicators.
In your case, 2 indicators do not fit into the norm: the free beta-hCG subunit is reduced and the risk of Down syndrome is high due to age.
Risks for Down syndrome are determined automatically by a special computer program, taking into account a number of factors.
A decrease in beta-hCG may indicate the presence of a chromosomal abnormality in the fetus in the form of Edwards syndrome, placental insufficiency, or threatening spontaneous miscarriage.
Any of the reasons requires immediate consultation with an obstetrician-gynecologist. If necessary, you will be prescribed the necessary therapy. In addition, genetic counseling is indicated for you, since you are at high risk for Down syndrome. According to indications, the geneticist will prescribe an additional study in the form of amniocentesis.
Hello! Help please, I didn’t donate blood, because the doctor said that it was too late, the last period was 16.05, according to the ultrasound they said no, they asked when the previous ultrasound was on 18.04 and they did it, all the data that is in the ultrasound: period 13, 5 weeks, ktr 75 mm, IVP 22 mm, heart rate 172 (she cried during the ultrasound, maybe that’s why) TVP 1.7, nasal bone +, blood flow in the venous duct pi 0.96, no tricuspid regurgitation, no CA markers, anatomy all +, limbs +, uterus and all without any features, cervix length Tvuzi 43 mm pharynx closed, DPM a uter dexpi- 2.56, a uter sinpi 1.95, this is all the data that is available, I want to take the genetic test, but the doctor said to wait for 2 screenings and then We’ll understand everything for him since they can’t set a deadline, can I pass the C grade relying on the deadline for this ultrasound and could it be that the deadline of May 16 is correct, and not from April 18, or should I listen to the doctor and wait for the second screening? The concern is that I took Reduxin 10 in the first weeks of pregnancy, as it turned out later, I’m afraid it might affect the baby, I drank it for a week, the doctor refrained from commenting on this matter, thanks in advance for your answer!
I am 25, weight 90, my first child is healthy.
Assuming your last period was 5/16, you should currently be 11-12 weeks gestational. If the last period is April 18, then the pregnancy period is 15–16 weeks.
To answer your question about the duration of pregnancy, you need to know:
- Have you had any problems with your menstrual cycle before?
- Have you had intermenstrual bleeding before?
- Do you have any underlying medical conditions such as hypertension, diabetes or thyroid disease?
- Do you have gynecological diseases, including cervical erosion and hormonal diseases?
- Did you take sex hormones before pregnancy?
- At what stage of pregnancy did you register for pregnancy? What happened during the gynecological examination?
- How was your last period? Have there been any changes to them?
- Did you take Reduxin 10 as prescribed and under the supervision of a doctor?
- Why didn't you protect yourself from pregnancy when taking Reduxin?
- How long did you take the drug?
- Your height?
The gestational age is determined based on the results of the first ultrasound screening. This is due to the fact that all fetuses at a gestation period of 10 weeks 6 days - 13 weeks 6 days are of a similar size.
Ultrasound and biochemical studies are carried out at gestational ages of 10 weeks 6 days - 13 weeks 6 days. In this case, blood is donated strictly after an ultrasound, which is associated with obtaining a result for a specific stage of pregnancy.
If you donate blood for chromosomal markers yourself, the data obtained may be incorrectly interpreted.
If we assume that normal menstruation was on April 18, then the following data is obtained.
- The CTE of the fetus at 13 weeks 5 days varies from 59–85 mm.
- The normal fetal heart rate at the 13th week of pregnancy is 147–171 beats per minute.
An increase in the indicator may be associated with your emotional state or indicate oxygen starvation of the fetus. It is necessary to know the condition of the placenta. If there are pathological changes in it, it is necessary to undergo appropriate therapy. The second option is to do a repeat ultrasound.
- TVP at 13–14 weeks of gestation should be 0.7–2.7 mm, the average value is 1.7 mm.
- The nasal bone should be clearly visible and be greater than 3 mm.
- Blood flow in the ductus venosus normally does not have a negative value or regurgitation.
- The cervix is 35–45 mm long, the internal and external os are closed.
Reduxin 10 is a drug for the treatment of obesity with central action. Has strict indications for use. During pregnancy, its use is prohibited, as there is no data on its safety for the fetus. Its use must be accompanied by strict contraception.
Hello! Thank you for your answer, the menstrual cycle is without delay, always on time, without discharge outside of menstruation, it so happened that I took hormones and everything was normal, the doctor prescribed reduxin to cause a positive trend towards weight loss, I took it for 7 days from 10.05 to 16.05, 16.05 menstruation went and lasted about 12 hours almost as usual, but less so, then they ended, I took a test on May 16 and it turned out to be positive, before taking reduxin I also took a test, that is, on May 6 and May 8 they were negative, I took hormones on April 6, everything was within the normal range, I wanted to take a C, but at the reception center they said that I myself could not take the test even for a fee and also advised a second ultrasound (that the data could be false positive or false negative) the doctor did not say anything about contraception (endocrinologist) I warned that there was an attempt to get pregnant just in March and the tests were negative, I specifically waited for my period on April 18 to understand whether there would be a delay or not, I did more than one test, I can’t even understand how this happened, after March they took contraception, most likely if there was a conception, it was on April 18 than on May 16, I think so, I’ll go for an ultrasound on August 15 to confirm or refute the date, so that all the parameters are accurately described for the nose, arms, legs, everything in general, then with this ultrasound I’ll go to a geneticist, since my local gynecologist can’t explain or say anything! Thank you!
Good afternoon Please help me decipher the tests of 1 screening. I am 31 years old, 3rd pregnancy, ultrasound term (CTR) is 12 weeks + 5 days, obstetric term is 12 weeks. Heart rate 155 st/m, CTE 64.0 mm, TVP 1.8 mm, nasal bone is determined. Free beta unit hHF 179.0 IU/l/4.171 MoM, PAPP-A 5.270 IU/l/1.722 MoM. Trisomy 21 basic risk 1:556 individual risk (basic + ultrasound + HD) 1:5616. trisomy 18 basic risk - 1:1359, ind. Risk 1:27185. Trisomy 13 base risk 1: 4264, index risk 1: 85276.
Among the screening data of the first trimester of pregnancy, you have normal indicators and deviations from the norm. Let's look at everything in detail.
An ultrasound examination includes not only the determination of CTE, TVP, fetal heart rate and visualization of the nasal bones, but also gives a general idea of the development of the fetus by indicating all its sizes and the condition of the placenta. In addition, after the study, a conclusion is given about the possibility of developing Down syndrome in the fetus. This indicator is calculated by an automatic program.
Let us analyze the ultrasonic indicators presented by you.
- The gestational age according to menstruation and ultrasound is the same and is 12–13 weeks.
- The fetal heart rate at 12–13 weeks of gestation varies from 150 to 174 beats per minute.
- The CTE of the fetus is 50–72 mm at 12 weeks 5 days.
- TVP normally ranges from 0.7–2.5 mm.
- The nasal bones are clearly visible and their thickness is more than 3 mm.
These indicators are within normal limits.
Let's analyze the results of biochemical screening.
Normally, the free beta-hCG subunit and PAPPA-A are in the range of 0.5–2.0 MoM.
The risks for all chromosomal abnormalities must be higher than 1:380. All indicators below this level fall into the high-risk group.
In your case, the risks of a chromosomal abnormality in the fetus do not fall into the high-risk group. However, beta-hCG and PAPPA-A levels are overestimated.
An isolated increase in PAPPA-A has no diagnostic value.
Increased concentrations of beta-hCG may occur:
In order to make sure that the child does not have a pathology, you need to immediately contact a gynecologist. After comparing all the data, the doctor will decide on further tactics for managing your pregnancy. You may need genetic counseling.
Hello, please tell me, I really need help deciphering the 1st screening.
I am 27 years old, my second pregnancy is planned, my first child is healthy. Last day of menstruation 08.05.
Ultrasound results (ultrasound period 11 weeks 3 days): CTR 46, BPR 18, heart rate 174, TVP 6.2. Biochemistry result: PAPP-A 0.907, hCG 0.717, risk tr.18 1:293, tr.21 1:1581, tr. 13 1:1153
The result of the second ultrasound on a different device after 6 days: CTR 59 (corresponding to 12 weeks 3d), BPR 19 (corresponding to 13 weeks), heart rate 165, TVP 4.6, nasal bone 1.7, Pi 0.90, VI ventricle 2.8, fetal features - preaxial polydantia of both hands cannot be excluded, umbilical cord 3 vessels. Conclusion: expansion of the TVP and the sixth ventricle as markers of CA.
Based on these data, is it possible to talk about any incurable diseases and what is my risk that the child will be born sick?!
The geneticist says that for such indications the pregnancy cannot be terminated and recommends undergoing a chorionic villus biopsy and a control ultrasound within a week.
Let's decipher the first screening study. The norms for the 11th–12th weeks of pregnancy are:
In your case, the marker of a chromosomal abnormality in the fetus is TVP.
According to the results of biochemical screening, the free beta-hCG subunit and PAPPA-A should be in the range of 0.5–2.0 MoM, and the risk values should be higher than 1:380.
According to the results of the study, you have an increased risk of having a child with trisomy 18, or Edwards syndrome.
Let's look at the second screening study. The growth of the child is noted according to the gestational age. The norms for the 12–13th week of pregnancy are:
- KTR - 51–59 mm;
- BPR - 18–24 mm;
- Heart rate - 150–174 beats per minute;
- TVP - 1.6–2.5 mm;
- nasal bone - clearly visualized, average value is 1.8 mm;
- VI ventricle - 10–15 mm.
Pathological indicators are expansion of the sixth ventricle and excess of the TVP value.
Another pathology according to ultrasound is preaxial polydactyly of both hands in the fetus. The pathological condition is manifested by doubling of fingers. This defect can be isolated, or it can occur as part of a chromosomal pathology in the fetus.
Gestational age 12w 6d according to KTR
Fetal heart rate 167 beats/min.
Ductus venosus PI 0.890
Chorion/placenta low on the posterior wall
Umbilical cord 3 vessels
Markers of fetal chromosomal pathology:
Nasal bone: determined; Tricuspid valve Doppler: normal
HCG 61.4 IU/L is equivalent to 1.805 MoM
PAPP-A 1.569 IU/l is equivalent to 0.528 MoM
Uterine artery PI 1.49 equivalent to 0.930 MoM
Trisomy 21 - basic risk 1:452/ind. risk 1:498
Trisomy 18 - basic risk 1:1110/ind. risk< 1:20000
Trisomy 13 - basic risk 1:3480/ind. risk< 1:20000
Preeclampsia before 34 weeks. pregnancy 1:4142
Fetal growth retardation up to 37 weeks of pregnancy 1:482
Spontaneous birth before 34 weeks of pregnancy 1:197
The gynecologist, as I understand it, drew attention to the risk of trisomy 21, in particular the too “close” index of ind. risk to the baseline. She also spoke about the research method by taking blood from a vein for DNA analysis (the procedure is not cheap). Please tell me whether there is any point in this study, which the doctor described, given such indications. Thank you very much in advance!
You have undergone the first fetal screening test in the form of an ultrasound and biochemical blood test.
I would like to clarify a few questions:
- Have you had any pregnancies before and how did they end?
- Are there any children in your family with Down syndrome or other chromosomal abnormalities?
- Ultrasound conclusion on the risk of having a child with Down syndrome.
- Concomitant pathology.
- Gynecological diseases.
We will analyze the data you provided.
The norms for 12–13 weeks of pregnancy are:
- KTR -mm;
- TVP - 1.6–2.5 mm;
- BPR -mm;
- ductus venosus - has no negative or reverse meaning;
- umbilical cord - 3 vessels;
- the nasal bone is clearly defined.
These indicators are within normal limits.
The location of the placenta can be any, however, it should be located high above the level of the cervix. At this stage of pregnancy, a low location of the placenta is allowed. As a rule, as pregnancy progresses, it rises upward. In order to avoid the threat of spontaneous miscarriage and bleeding, I recommend that you abstain from sexual activity until the next ultrasound.
Biochemical screening allows you to conduct a blood test for markers of chromosomal abnormalities in the fetus: trisomy 13, 18 and 21 pairs of chromosomes.
Normally, the levels of free beta-hCG subunit and PAPPA-A should be from 0.5 to 2.0 MoM.
The risks for a chromosomal abnormality must be higher than 1:380 for all indicators.
According to the results of the study, you are in a high-risk group for premature birth before 34 weeks of pregnancy, which requires increased attention from a doctor.
The indicator for trisomy 21 pairs of chromosomes, or Down syndrome, is close to the basic and individual risk, but does not fall into the high-risk group.
Perhaps your doctor had a different research method in mind, since you underwent non-invasive prenatal diagnostics for congenital chromosomal pathologies. Most likely, the gynecologist suggested that you undergo biochemical screening in the second trimester of pregnancy to exclude pathology in the fetus.
You should check the details with your treating gynecologist, who, if indicated, will prescribe additional research methods for you.
I found the name of the procedure:
Non-invasive prenatal diagnostics for congenital chromosomal pathologies
Help me figure out the fetal heart rate is 153 beats/min. KTR 73.0mm. TVP 1.90 mm. Free beta subunit of hCG - 101.20 IU/l/2.715 MoM PAPP - 3.208 IU/l/0.513 MoM. Trisomy 21 base risk 1:699. Individual risk 1:361 Trisomy 18. basic risk 1:1780 individual risk 1:35604. Trisomy 13 base risk 1:5564 individual risk 1:111279
I would like to communicate with you via email, if it’s not difficult, please write
On July 11, 2017, blood was drawn for 1 screening and an ultrasound examination of the fetus was performed. The ultrasound specialist set a deadline of weeks. KTR - 52mm, HR-160, TVP - 0.7mm, the nasal bone is determined (I can even see it from the photo). On August 18 (more than a month later!) the blood results finally arrived - hCG - 76.9 IU/l, PAPPA - 0.373 IU/l. They write the risks of Trisomy 21 - 1: 222 (area of attention), Trisomy 1: 706 (area of attention), trisomy 13 1: 1722. Send to a geneticist. This is the first child, there are no hereditary diseases, no abnormalities in the family either. I am a healthy person in all respects. BUT: I know exactly the day when my husband and I actually tried. Because, due to family circumstances (illness of the husband’s mother), this could not happen on any other day. And in principle, the child is conscious. This is May 1, 2017. Accordingly, the period cannot be more than 10 weeks, it can be 9 weeks and 5-6 days, for example (conception does not always occur on the day of PA). Among other things, if the term is set according to the coccygeal-parietal size, then we have a peculiarity in our family - my own father was born with a weight of 5.2 kg (and they have all 3 children with the same weight), my mother is 4.2 kg. I'm 3.3kg - normal weight. But still, everyone in the family was born large. I am very worried about possible deviations. But, as far as I understand, with a shorter actual period, hormone levels should be lower. And our TVP is small.
In order to answer your question correctly, the following information is required:
- First day of last menstruation.
- Do you have a regular menstrual cycle? Its duration.
- Have you done ovulation tests? If yes, which ones?
- A complete picture of ultrasound screening with a conclusion on the risk of developing a child with Down syndrome.
- Free beta-hCG and PAPPA-A subunit results in MoM study units. Other indicators are individual for each laboratory and may differ significantly.
Since it is not known when the first day of your last period was, it can be assumed that you ovulated early. This also explains the difference of 7 days between your estimated gestational age and the ultrasound screening data.
An ultrasound examination is taken for the gestational age. Up to 12 weeks of gestation, fetal growth is the same. Individual growth begins after the 12th week.
For 11–12 weeks of pregnancy, ultrasound standards are as follows:
- KTR - 34–59 mm;
- Fetal heart rate - 150–174 beats per minute;
- TVP - 0.8–2.2 mm, but not more than 3 mm;
- The nasal bones at the 11th week of pregnancy are clearly visualized, but not measured.
According to the risks after a biochemical study, all indicators should be more than 1:380. The data below fall into the high-risk group.
In your case, genetic counseling is necessary. If indicated, you will be asked to undergo an invasive fetal examination to determine chromosomal pathology.
Please help me decipher the results! I am 27 years old. according to the monthly period, 12 allotments and 4 days at the time of delivery of hair 1, and according to the ultrasound on the same day, 13 weeks. and 2 days. KTR 67 neck fold 2.6 mm nasal bone 2.1 mm. result RAPP-A 6, 13 speed MoM 1.79, fb-hCG 42, 7 speed MoM 1.33. Biochemical risk 1:5252, double test 1:8589 Age risk 1:872. Trisomy 13/18 + NT 1:10000
There is not enough data to fully decipher the condition of the fetus. Need to know:
- a complete picture of ultrasound screening indicating all dimensions of the fetus: BPD, abdominal circumference, thigh length;
- conclusion based on the results of ultrasound screening indicating the risks of developing Down syndrome in the fetus;
- Fetal heart rate;
- condition of internal organs;
- number of umbilical cord vessels;
- size, condition and location of the placenta;
- your medical history data.
The normal difference in the timing of pregnancy according to ultrasound screening and menstruation is considered to be within 7 days. The gestation period depends on the moment of ovulation, which can be not only in the middle of the cycle, but also early or late.
The following indicators are considered normal values for the first ultrasound screening at 13–14 weeks of pregnancy:
- KTR - 54–78 mm;
- The TVP, or cervical fold, ranges from 1.7–2.7 mm;
- The nasal bone is clearly visible on ultrasound, and its thickness ranges from 2 to 4.2 mm.
According to the results of biochemical screening, the free beta-hCG subunit and PAPPA-A should be in the range from 0.5 to 2.0 MoM, other units of measurement are individual for each laboratory. Risks for all indicators of chromosomal abnormalities are normally higher than 1:380.
To obtain accurate information about the condition of the fetus, you need to contact an obstetrician-gynecologist at your place of residence. Based on the totality of all data: medical history, ultrasound and biochemical screening, the doctor will answer all your questions.
Good afternoon. Help me understand the screening results. Ultrasound and blood tests 12 weeks 5 days Ultrasound data: CTE 69mm BPR 21mm Fetal heartbeat: determined, heart rate 166 beats/min. PI: 0.91 Thickness of the nuchal space: 1.6 mm Nasal bone visualized: 2.1 mm Fetal anatomy: Bones of the cranial vault: b/o Brain structures: M-echo: b/o Spine: b/o Stomach: b/o Anterior abdominal wall: b/o Choroid plexuses: b/o IV ventricle: Four-chamber section of the heart: b/o Bladder: b/o Upper and lower extremities: b/o Yolk sac: not visualized Amnion: features: b/o Predominant localization of the villous chorion: posterior wall of the uterus, thickness 13 mm Structure of the orion: b/o Condition of the uterine walls: b/o Ovaries: in the right corpus luteum 23 mm Conclusion: Ultrasound signs of progressive pregnancy, 13 weeks Blood test data: PRISCA I trimester test Associated with pregnancy protein A (PAPP-A): 0.95 mIU/ml Free b-subunit 26.40 ng/ml
For a gestational age of 12–13 weeks, the following are considered to be the norms:
- KTR - 50–72 mm;
- BPR - 18–24 mm, average value is 21 mm;
- Fetal heart rate - 150–174 beats per minute;
- PI - the indicator should have a positive value with the absence of regurgitation;
- TVP - 0.7–2.5 mm, the average is 1.6 mm;
- nasal bone - clearly visualized, its thickness varies from 2 to 4.2 mm;
- fetal anatomy - without features;
- chorion thickness - 10.9–19.8 mm;
- the structure of the chorion is without features, located high above the internal os;
- amnion - without features;
- corpus luteum - 10–30 mm.
The data you provided is within normal limits.
To make a conclusion, it is necessary to know the risk of Down syndrome in the fetus based on the results of ultrasound screening, which is calculated automatically by a special computer program based on all the data obtained and the woman’s medical history.
There is very little data to decipher the results of biochemical screening. Need to know:
- indicators of the free subunit of beta-hCG and PAPPA-A in the MoM unit of measurement, which is universal for all laboratories and normally ranges from 0.5 to 2.0;
- when indicating other units of measurement, such as mIU/ml or ng/ml, it is necessary to give the values of normal values, which are different for each laboratory and are indicated when issuing results;
- risks due to the presence of chromosomal abnormalities in the fetus: trisomy 13, 18 and 21 pairs of chromosomes, which are normally higher than 1:380.
Good afternoon First pregnancy
26 years. Pregnancy 12 weeks. 6 days. Ultrasound screening: CTE 83mm, BPR 25mm, heart rate 155 beats/min, TVP 2.1mm, nasal bones 2.5mm. Biochemistry results: hCG 44.78 IU/l/ 1.430 MoM, PAPP-P 4.456 IU/l- 0.646 MoM. What is the likelihood of Down syndrome
Hello, I’m 31 years old, I had genetic screening done in the 1st trimester, these are the results, help me figure it out:
2nd pregnancy, 62.5 kg, at the time of screening 30 years 11 months, concomitant disease chronic autoimmune thyroiditis.
Last menstruation 17.05. Ovulation 05.06. (Late ovulation, the period is a little less than what is written)
Ultrasound: CTE 43.5. Nose bones 2.3mm. Heart rate 172 beats/min. The thickness of the collar space is 1.5 mm.
Gestation period 11.1 weeks
free beta-hCG 200. 4.01 MoM;
PAPP-A 1.19. 0.69MOM
Biochemical + NT 1:86
Double test >1:50
Age risk 1:565
Trisomy 18+NT<1:10000
Now I'm 16 weeks pregnant, an ultrasound scan was done, everything was normal, no abnormalities. We took an AFP test and 2nd trimester screening, we are waiting for the result.
Thanks for the answer.
There are a few important questions left for you:
- How was ovulation checked? What tests were used?
- How did your first pregnancy end?
- Are you taking Levothyroxine, Euthyrox or others tablets for chronic autoimmune thyroiditis?
- Are you seeing an endocrinologist?
- What are the TSH levels?
- Do you have hypothyroidism?
- Fruit sizes: BPR, OJ, DB.
- Conclusion on the risk of Down syndrome based on ultrasound screening results.
- Have you been referred to genetic counseling?
- Have you or your close relatives had children with chromosomal abnormalities?
For a gestational age of 11–12 weeks, the norm is in the range of:
- KTR - 42–50 mm;
- nasal bones are clearly visualized;
- TVP - 0.8–2.2 mm.
The biochemical parameters of the first screening, free beta-hCG subunit and PAPPA-A, normally vary from 0.5 to 2.0 MoM.
Your beta-hCG level is 2 times higher than normal. This may be due to:
Risks for chromosomal abnormalities are normally above 1:380 for all indicators.
According to a biochemical study, you are in a high-risk group for having a child with a chromosomal pathology.
I recommend waiting for the results of the second screening, contacting your obstetrician-gynecologist and, if indicated, a geneticist. The question of whether it is advisable to visit a geneticist is decided individually for each woman.
Good afternoon I ask for your advice. 2nd pregnancy, 13 weeks. and 3 days. 40 years. Weight 70.4. According to ultrasound and blood: CTR 72 mm, BPR 22 mm, LZ 29 mm, OG 82 mm, coolant 71 mm, femur length 11 mm. Heart rate 158. TVP 2.1 mm. The nasal bones are visualized, 2.6 mm. The thickness of the chorion is 19 mm, along the posterior wall of the uterus. An interstitial-subserous myomatous node with a diameter of 47 mm is located along the posterior wall of the uterus. Hypertonicity of the myometrium along the anterior wall of the uterus. Free beta subunit of hCG 23.30 IU/l/0.658 MoM. PAPP-A 2.170 IU/l/ 0.616 MoM. Baseline risk: trisomy 21 - 1:69. Trisomy 18 - 1: 174. Trisomy 13 - 1: 545. Individual. risk of trisomy 21 - 1:827. Trisomy 18 - 1: 3486. Trisomy 13 - 1: 2476. I understand that there is always a risk, no one is immune. But I would not like to do amniocentesis and similar tests. Thank you in advance.
Hello, I need your advice
According to monthly period 12 weeks, according to ultrasound 14 weeks.
Beta subunit hCG: 13.68 IU/l/ 0.455 MoM
PAPP-A: 1.574 IU/l/ 0.426 MoM
Trimosomy 21: baseline: 1:504
Trimosomy 18: baseline: 1:1328
Trimosomy 13: baseline: 1:4139
Risk of hyperthesia disorders
Risk of developing preeclampsia before 34 weeks 1:2017
Fetal growth restriction up to 37 weeks 1:282
Doppler ultrasound of the uterine arteries:
Mean arterial pressure 83.4 mm Hg. equivalent to 0.960 MoM
Mother's age 32 years
There are a few questions left for you:
- Do you have regular periods?
- If the menstrual cycle is irregular, the minimum and maximum dates for the onset of menstruation.
- According to the results of the ultrasound, the gestational age is exactly 14 weeks or, for example, 13 weeks 6 days.
- Have you ever had a pregnancy and how did it progress? Were there any complications during pregnancy and childbirth?
If the gestational age is 14 weeks or more, ultrasound screening is not informative for identifying the risk of Down syndrome in the fetus.
According to the results of the first ultrasound screening at 14 weeks of pregnancy, the indicators should be within the following limits:
- Heart rate - 146–168 beats per minute;
- KTR - 63–89 mm;
- TVP - 0.7–2.7 mm;
- thigh length - 9.0–15.8 mm;
- blood flow in the venous duct - has a positive value in the absence of reverse.
Based on the results of biochemical screening, the indicators should be within the following limits:
- Free beta-hCG subunit - 0.5–2.0 MoM;
- PAPPA-A - 0.5–2.0 MoM;
- the risks of developing abnormalities in the fetus are higher than 1:380.
You are at increased risk of fetal growth restriction before 37 weeks of pregnancy. This means that with the same indicators, this risk to the fetus is in one in 282 women.
Hello! Please consult.
Based on the results of the first screening at 12 weeks and 4 days
hCG was 0.45 mOhm
HCG free b-subunit 18
Trisomy 21: basic
Trisomy 18: basic
Trisomy 13: basic
I was not satisfied with the hCG level and a few days later I took it again..
Term 13 weeks and 1 day
Free b-subunit 15
HCG 59026.47 mIU/ml
PAPP-A plasma protein 6.56 IU/ml
Please tell me, is it normal that hCG decreases? Or does this mean something?
I will be very grateful for the answer..
- Have you had a consultation with your doctor about the research results?
- What were the indicators of ultrasound and biochemical screening?
- The risk value for trisomy 18 pairs of chromosomes according to the results of a biochemical blood test.
- Condition of the placenta.
- Your general condition: pain in the lower abdomen, presence or absence of bloody discharge from the genital tract, toxicosis.
According to ultrasound screening at 12–13 weeks of pregnancy, the normal indicators are:
You do not indicate the values of the first biochemical screening indicators, except for beta-hCG. Without data, it is impossible to give a conclusion.
The indicators should be as follows:
A reduced beta-hCG level can be observed with:
I recommend that you immediately contact a gynecologist at your place of residence to obtain reliable information on the research results. If indicated, you will be recommended to consult a geneticist with additional research methods.
Good afternoon. Help me figure it out, I’m really worried. I am 33 years old. Pregnancy 2. Weight 46 kg. 1 - pregnancy ended in childbirth (baby is healthy). An ultrasound was done by a geneticist at 12 weeks 4 days; according to the results, all indicators were normal, no abnormalities were found in the fetus. BUT: there is a marginal placenta previa. At 12 weeks 6 days I did a biochemical screening: according to the results, PAPP-A (mom) was 1.78, and free hCG (mom) was 2.21. How to understand this? (very worried)
- How does a real pregnancy proceed?
- Is there toxicosis?
- Is there pain in the lower abdomen or bloody discharge from the genital tract?
- Why did you have your first ultrasound done by a geneticist? Was there evidence for this?
- How was your previous pregnancy and childbirth?
- Do you have any concomitant diseases such as diabetes or other pathologies?
Based on the results of biochemical screening, the following data should be normal:
- indicators of free beta-hCG subunit and PAPPA-A - 0.5–2.0 MoM;
- risks for all indicators are higher than 1:380.
In your case, there is a slight increase in beta-hCG. This indicator may increase if:
Marginal placenta previa is the location of the placenta in the area of the internal os, but does not extend beyond it.
Diagnosed marginal placenta previa in the first 16 weeks of pregnancy requires increased attention from a gynecologist. If there are no complaints, bloody discharge from the genital tract, and the patient’s general condition is satisfactory, management is carried out on an outpatient basis.
If complaints arise, hospitalization is carried out in a hospital.
- visiting a bathhouse, sauna;
- performing any physical activity;
- sexual acts.
As a rule, with the growth of the uterus, the placenta rises upward, which is determined by the second ultrasound. If the placenta does not rise, the patient is managed according to treatment protocols.
Good night. Help me decipher the results, please! Gestational age at the time of screening was 12 weeks 2 days (32 years):
T 21 B 1:473 I 1:179
T 18 B 1:1129 I 1:17730
T 13 B 1:3550 I 1:14695
free beta hCG 90.90
Uterine arteries PI 1.740
Cervical canal length 33
At 12–13 weeks of pregnancy, ultrasound examination indicators are:
- Heart rate - 150–174 beats per minute;
- KTR - 51–59 mm;
- TVP - 0.7–2.5 mm;
- BPR - 18–24 mm;
- exhaust gas - 58–84 mm, average value - 71 mm;
- Coolant - 50–72 mm.
The data you provided is within normal limits.
You indicate biochemical screening data in the data, the interpretation of which is indicated individually for each laboratory. The international unit of measurement for free beta-hCG subunit and PAPPA-A is MoM, which is common to all laboratories. Indicators from 0.5 to 2.0 MoM are considered normal.
Risks based on the study results for all indicators should be higher than 1:380. Indicators less than 1:380 are considered high risk.
In your case, you are in a high-risk group for having a child with trisomy 21 pairs of chromosomes, or Down syndrome according to an individual calculation. It can be assumed that you or your close relatives had children with Down syndrome.
In order to determine whether your child is sick, it is necessary to undergo genetic counseling. If indicated, you will be offered amniocentesis or other invasive testing. Based on the results of a fetal DNA test, the presence or absence of genetic abnormalities will be determined.
Good afternoon. I would like to get a little advice. I am 33 years old. Gestation period: weeks. Screening results: PAPP-A - 0.473 mΩ, BHG - 1.494 mΩ. Risk for trisomy 21 1:189. Ultrasound examination revealed no signs of congenital malformation or markers of chromosomal abnormalities.
According to ultrasound at 12.6 weeks, TVP was 2.2 mm, nasal bone was 2.0 mm, heart rate was 158 beats per minute. The geneticist said that there is a risk, and an ultrasound should be done before 20 weeks. To be honest, I don’t quite understand, there is no risk based on the ultrasound, but there is a risk based on the blood test. I did everything in one day. They were completely confused and terrified. I'm worried that the puncture will lead to a miscarriage.
There is not enough data to reliably answer your question. It is necessary to indicate:
- What kind of pregnancy is it?
- How previous pregnancies ended, if any.
- In the case of childbirth, how the pregnancy proceeded, whether there were any abnormalities in the fetus according to the results of the study, whether there was any pathology in the child.
- If there were abortions, were any of them abortions for medical reasons?
- Are there any children with Down syndrome among your relatives?
- A complete ultrasound picture indicating all the data: the size of the fetus, the condition of the placenta, a conclusion on the risk of Down syndrome.
Based on the data you provided, we can draw the following conclusions.
The norm for the first ultrasound screening at 12–13 weeks of gestation is the following data:
The biochemical screening standards are:
- free beta-hCG subunit and PAPPA-A - 0.5–2.0 MoM;
- risks for all indicators are above 1:380.
In your case, based on all the data, the fetus is at high risk for Down syndrome. This means that a child with a chromosomal pathology can be born to one woman out of 189 with the same data as you.
If a geneticist believes that you have indications for amniocentesis, you should listen and undergo the procedure.
Amniocentesis is performed under ultrasound guidance. Complications occur in very rare cases.
Help me please. I took tests at 11 weeks and 6 days. Ultrasound results:
KTR-52, BPR-17, ChSS-164, TVP - 1.6 (MoM 1.15), Spout - 1.6
BetaHCG-71.5 ng/ml (cor. MoM = 1.54)
PAPP-A - 1.29 mIU/ml (cor. MoM = 0.48)
I am 29 years old, first pregnancy, fetus 1
Biochemical risk+NT 1:760
Double test 1:265
Age risk 1:681
Trisomy 13/18+ NT<1:10000
You have undergone a double screening test for the first trimester of pregnancy, which includes:
- ultrasound examination of the fetus;
- biochemical blood test.
There is very little data to give a conclusion about the development of your pregnancy. Need to know:
- Regularity of the menstrual cycle.
- Do pregnancy dates match according to menstruation and ultrasound.
- Were there any children in the family with developmental anomalies, including Down syndrome?
- Full description of ultrasound screening:
- head circumference;
- abdominal circumference;
- thigh length;
- Are the cerebral hemispheres symmetrical?
- brain structure;
- condition of internal organs;
- number of vessels in the umbilical cord;
- venous blood flow;
- condition of the placenta;
- conclusion about the risk of Down syndrome in the fetus.
- According to the results of biochemical screening:
- risks due to chromosomal abnormalities.
At 11–12 weeks of pregnancy, the norms during the first ultrasound screening should vary within the following limits:
- KTR - 40–58 mm;
- BPR - 13–21 mm;
- Heart rate - 153–177 beats per minute;
- TVP - 0.8–2.2 mm, the average value at 11 weeks and 6 days is 1.6 mm;
- the bones of the nose are clearly visualized, their thickness begins to be determined from the 12th week of gestation.
Based on the results of biochemical screening, the indicators should be:
- free beta-hCG subunit and PAPPA-A - 0.5–2.0 MoM;
In your case, there is an increased risk of having a child with a chromosomal abnormality. This means that with the same indicators as yours, it is possible for 1 out of 265 women to have a child with the pathology.
I recommend that you consult a gynecologist to choose further tactics for managing your pregnancy. You may need genetic counseling, the indications for which can only be determined by your attending physician.
Good afternoon I kindly ask you to help me understand the ultrasound examination. I am 34 years old. Second pregnancy and second birth. Term 12 weeks 3 days. How do I understand that I have deviations in the nasal bone and TVP? Somewhere there are still indicators written, not the norm. Could these also be developmental deviations? What can be the consequences of these fetal abnormalities? Very worried.
The cranial vault is normal;
TVP 2.4 (Normal up to 2.37)
Anterior breast wall - normal
Bladder is normal
Extremities N-norm, B-norm
ChSSud. 1 min.
SVD of the yolk sac is normal
Section through 3 vessels - unclear
I would like to receive more information in order to give a correct conclusion about the development of your child:
- Features of the first pregnancy.
- What were the indications for caesarean section? The operation was performed either planned or emergency.
- What is the conclusion regarding the risk of Down syndrome based on the results of ultrasound screening?
- Have you undergone biochemical screening in the first trimester of pregnancy?
- Have you been prescribed genetic counseling?
- Were there chromosomal pathologies in the family?
- Do you have any complaints of pain in the lower abdomen?
Based on the data you provided, the following conclusions can be drawn.
During pregnancy 12–13 weeks, indicators based on ultrasound screening results should be within the following limits:
- KTR - 50–72 mm;
- TVP - 0.7–2.5 mm;
- nasal bones - 2–4.2 mm;
- Heart rate - 150–174 beats per minute;
- blood flow in the ductus venosus is positive, has no reverse;
- scar thickness - more than 5 mm;
Differences in ultrasound standards may be due to the class of ultrasound diagnostic device. In this case, it is necessary to focus on the values of normal indicators for a specific laboratory.
If indicated, you will be asked to undergo a consultation with a geneticist with an invasive research method.
In addition, you need to undergo biochemical screening, which will allow you to identify risks for a number of chromosomal pathologies.
Good afternoon! Help me understand the screening results. period 12 weeks.3 days.
chorion: high on the anterior wall
umbilical cord 3 vessels
Biochemistry of maternal serum:
PAPP-A 1.258 IU/l/0.378 MoM
Expected risk of Trisomy 21,18,13:
trisomy 21: base risk 1:996; individual risk 1:19913
trisomy 18: base risk 1:2398; individual risk 1:3064
trisomy 13: base risk 1:7533; individual risk 1:21322
Please clarify a few important questions:
- Your age.
- What kind of pregnancy is this?
- Full picture of ultrasound with a conclusion on the risk of Down syndrome in the fetus.
- Thickness of the nasal bone according to ultrasound.
- Your general condition, complaints of pain in the lower abdomen, bleeding from the genital tract or others.
For a gestational age of 12–13 weeks, ultrasound screening indicators should be as follows:
- Heart rate - 150–174 beats per minute;
- KTR - 47–67 mm;
- TVP - 0.7–2.5 mm;
- BPR - 18–24 mm;
- nasal bone - clearly visualized, more than 3 mm.
The nasal bone begins to be visualized from the 11th week of pregnancy, and its thickness begins to be assessed from the 12th week of gestation.
The ultrasound examination data you indicated are within normal limits.
The results of a biochemical study should normally be as follows:
- free beta-hCG subunit and PAPPA-A - 0.5–2.0 MoM;
- risks for chromosomal abnormalities - more than 1:380.
In your case, according to the results of a biochemical blood test, a decrease in beta-hCG and PAPPA-A is noted.
A decrease in beta-hCG may occur with:
- Edwards syndrome;
- ectopic pregnancy;
- placental insufficiency;
A decrease in PAPPA-A may occur with:
- Cornelia de Lange syndrome;
- Down syndrome;
- Edwards syndrome;
- high risk of spontaneous miscarriage.
Hello, Irina Vyacheslavovna! Please help me identify the risks. I am 35 years old, this is my fifth pregnancy (two children, two miscarriages). At the first screening of 12 weeks 6 days, an ultrasound revealed a golf ball, heart rate 160, TVP 1.8, nasal bone 2.2, biochemistry-hCG 0.306. PPAR 2.002Mohm. The base risk for Down Syndrome is 1:225. individual 1:4498. I got to see a geneticist only after the second ultrasound screening (22 weeks). On ECHO-CG of the fetus there is only a 2mm MCA ball, everything else is without pathologies. The geneticist immediately told me that I was at high risk for diabetes. And in my case she considers the risk to be basic! Wrote -0.5 percent. I’m very worried, but do you think it’s worth it?
P.S. During the first screening, I took Utrozhestan (400 mg per day), had breakfast at 6 am, and took the test at 12.00. Could there be an error?
In order to talk about your child's condition, you need to know:
- Timing of spontaneous miscarriages.
- Has the cause of the miscarriages been determined?
- What kind of examination, treatment and planning of subsequent pregnancy was there after miscarriages?
- Age of the child's father.
- Did you have any signs of threatening spontaneous miscarriage at the time of the screening test in the form of pain in the lower abdomen or bloody discharge from the genital tract?
- The reason for the late appearance to the geneticist.
- What were the geneticist’s recommendations after the consultation?
- Full picture of ultrasound in the first and second trimesters.
- Have you done a second biochemical screening?
- Have you been adjusted according to the results of a biochemical analysis for taking Utrozhestan?
Golf ball syndrome is an ultrasound marker of a hyperechoic intracardiac focus. The average size of the formation is 1–6 mm. Most often found in the papillary muscle of the left ventricle. Golf balls are microcalcifications in muscle tissue.
A golf ball is often one of the markers of Down syndrome. However, microcalcifications can also occur during normal fetal development.
By the time of birth, in most cases, the golf ball disappears on its own.
At 12–13 weeks of pregnancy, the norms for ultrasound screening are as follows:
- Heart rate - 150–174 beats per minute;
- TVP - 1.6–2.5 mm;
- nasal bones - clearly visualized, 2–4.2 mm.
Blood is donated for biochemical screening strictly on an empty stomach. It is not advisable to even not drink water. When taking a hormonal drug, you had to clarify this when taking the test. The results of the study had to be adjusted.
According to the results of a biochemical study, the norms are as follows:
In your case, there is a decrease in beta-hCG, which may be due to:
- Edwards syndrome;
- ectopic pregnancy;
- placental insufficiency;
- high risk of spontaneous miscarriage.
Taking Utrozhestan may suggest that you were at risk of pregnancy loss.
I cannot rule out pathology in the fetus. Only invasive research in the form of cordocentesis, chorionic villus biopsy or amniocentesis, depending on the gestational age, can be reliable.
You missed the deadline when you could have done an additional examination.
With the same results as yours, the risk of having a child with Down syndrome is 1 in 225 births.
Hello, help me understand the results! I am 35 years old, 6 pregnancies, 2 children, 3 abortions. Ultrasound 12.4 weeks. Heart rate 154, CTR 59, TVP 1.63, ductus venosus 1.21, nasal bone 1.94. Free beta subunit hCG 30.9 IU/l equivalent to 0.836 MoM, PAPP-A 0.096 IU/l equivalent to 0.167 MoM. Trisomy 21 base risk 1:233 individual 1:616, trisomy base risk 1:557 individual 1:356, trisomy 13 basic rtsk1:1751 individual 1:1706
I would like to receive answers to the following questions:
- Have you or your close relatives had children with chromosomal abnormalities?
- There were abortions for medical reasons.
- Age of the child's father.
- Complaints characteristic of a threatened spontaneous miscarriage: pain in the lower abdomen, spotting.
For a gestation period of 12–13 weeks, ultrasound screening standards are as follows:
- Heart rate - 150–174 beats per minute;
- KTR - 49–69 mm;
- TVP - 0.7–2.5 mm;
- ductus venosus - positive value with no reverse values;
- nasal bone - 2–4.2 mm.
Normal data for biochemical screening are:
- beta-hCG - from 0.5 to 2.0 MoM;
- PAPPA-A - from 0.5 to 2.0 MoM;
- risks for all indicators are more than 1:380.
A decrease in PAPPA-A levels can occur with:
- Cornelia de Lange syndrome;
- Down syndrome;
- Edwards syndrome;
- threat of premature termination of pregnancy.
In your case, you are at high risk of having a child with trisomy 21, or Down syndrome, and 18, or Edwards syndrome, chromosome pairs.
Hello! The indicators are as follows:
free beta hCG 4.83 IU/l 0.123 MoM
PAPP-A 1.010 IU/l /0.355 MoM
Trixomy 21 basic 1:962 individual 1:19247
Trixomy 18 basic 1:2307 individual 1:201
Trixomy 13 basic 1:7248 individual 1:6131
Pregnancy 12 weeks 6 days
All other ultrasound parameters are normal
Hello, I'm 35 years old. I did genetic screening and the result was (high risk of diabetes based on biochemistry only). according to the ultrasound result as of October 05, 2017. -11 weeks 5 days, CTE 50.7 mm, heart rate 162, nuchal translucency thickness 1.5 mm, fetal nasal bone length 2.1 mm, yolk sac SVD 4 mm, age-related risk 1/336, risk limit 1/250, calculated risk 1/236. At the time of the test, I was and still am taking Duphaston, 1 tab twice a day, there was a risk of spotting from August 11 to September 3, 2017, and no one warned me that the test was being taken on an empty stomach. FB_DBS (Conc. 129.0) (PTO corr. 2.32). But at the same time, the doctor says that perhaps due to duphaston the hormone is increased..... I didn’t understand her, I couldn’t even really explain. Don't know. maybe not exactly. etc. I had a terotoxic goiter and was tested for hormones on October 21, 2017. TSH showed 6.18 when the norm is 0.27-4.20. Could this analysis also have an impact? Please help me, explain to me what and how. In advance, thank you very much for any answer.
- Have you had any pregnancies and how did they end?
- Were there any children in the family with Down syndrome or other chromosomal abnormalities?
- Full picture of ultrasound screening.
- Complete picture of biochemical screening.
The norms for indicators for 11–12 weeks of pregnancy are:
- KTR - 39–57 mm;
- Fetal heart rate - 153–177 beats per minute;
- TVP - 0.8–2.2 mm;
- the average length of the nasal bones is 1.4 mm, while the bones are clearly visualized, and their size begins to be assessed from the 12th week of gestation;
- SVD of the yolk sac - 4.2–5.9 mm;
- risks - more than 1:380.
Based on the results of biochemical screening, the norms are:
- free beta-hCG subunit and PAPPA-A - 0.5–2.0 MoM;
- risks for chromosomal abnormalities - more than 1:380.
Elevated beta-hCG levels may result from:
- high risk of Down syndrome in the fetus;
- severe toxicosis;
- endocrinological pathology, including diabetes mellitus in the mother.
Indicators may change if the analysis is performed incorrectly, if it was not taken on an empty stomach.
If you took the test on an empty stomach, but took Duphaston, it was necessary to notify the laboratory assistant so that the results of the biochemical study could be adjusted.
- visit an endocrinologist to adjust and prescribe the necessary treatment for thyrotoxic goiter, followed by re-testing;
- be observed during pregnancy not only by a gynecologist, but also by an endocrinologist;
- undergo genetic counseling;
- undergo a second biochemical and ultrasound screening;
- if indicated, undergo invasive diagnostics in the form of amniocentesis to accurately identify the condition of the fetus.
1. The first pregnancy was IVF / currently natural.
2. Indications for caesarean section were due to the fact that the pregnancy was IVF, but labor began
unexpectedly at 37 weeks, everything was as expected and the waters broke and contractions began. As a result, I had an emergency operation; the doctor didn’t like the discharge (dark brown, + the cervix did not open). There was 1 artery in the umbilical cord (there was no fetal hypoxia during pregnancy).
3. There were no chromosomal pathologies in the family.
4. On the days of screening, there was short-term pain in the lower abdomen.
I am 34 years old. Second pregnancy. 1st child is healthy 4 years old.
The cranial vault is normal;
Nasolabial triangle is normal
TVP 2.4 (Normal up to 2.37)
Anterior breast wall - normal
Bladder is normal
Extremities N-norm, B-norm
Heart rate - 160 beats. 1 min.
Blood flow in the ductus venosus PI - 1.14
4-chamber section of the heart - normal
SVD of the yolk sac is normal
Section through 3 vessels - unclear
Predominant localization of the chorion: anterior wall
The structure of the chorion is not changed
Number of vessels in the umbilical cord -3
The place of attachment of the umbilical cord to the placenta from the edge is 3.3 mm, normal.
Features: hypertonicity along the anterior wall. mimometer thickness. in the area of the scar 6.7 mm.
Conclusion: the fetus corresponds to 12.5 weeks.
The next day, I went to another laboratory and another specialist to do an ultrasound. October 18 12 weeks 4 days. Results:
Cranial vault without features
Butterfly without features
Stomach without features
Anterior breast wall without features
Bladder/kidneys without features
Facial angle without features
Spine without features
Limbs without features
Ductus venosus without features
Conclusion: The fetus corresponds to 12.6 weeks of pregnancy. Risk of CA.
Same day tests:
Biochemical risk +NT on the date of sample collection 1>50 above the cut-off threshold
Age risk at sample collection date 1:284
Triosomy 13/18+NT 1:5396 below the cutoff.
PAPP-A 3.45 mlU/ml 0.76 Speed
fb-hCG 72.8 ng/ml 1.80 Speed
At 3-4 obstetric weeks, I took an X-ray of my nose due to a severe runny nose, not knowing about the pregnancy. The gynecologist was informed about this from the 5th week of pregnancy. At the moment I somehow managed to get a referral to a geneticist. But for some reason she thinks that my indicators are low, although as I understand it, the biochemical risk +NT on the date of sample collection is 1>50 above the cut-off threshold - this is a high risk of having a child with Down syndrome? And is the age-related risk also high? Or am I missing something? Thanks for the answer.
For the week of gestational age, the norms are as follows:
- KTR - 50–72 mm;
- BPR – 18–24 mm;
- TVP - 0.7–2.5 mm;
- nasal bones - 2–4.2 mm;
- Heart rate - 150–174 beats per minute;
- blood flow in the venous duct is positive and has no reverse.
According to the results of the second ultrasound, there are deviations in the form of increased TVP and a decreased value of the nasal bones. This may be evidence of a chromosomal abnormality in the fetus.
Let's look at the results of biochemical screening:
- free beta-hCG subunit and PAPPA-A – 0.5–2.0 MoM;
- the risks of a chromosomal abnormality are higher than 1:380.
Beta-hCG and PAPPA-A are within normal limits in your case.
According to research results, you are at risk for having a child with a chromosomal abnormality.
In your case, a consultation with a geneticist is required, who can make the following recommendations:
- undergo an additional second screening: biochemical and ultrasound;
- undergo invasive diagnostics of the fetal condition:
- amniocentesis - at 16–20 weeks of pregnancy;
- cordocentesis - at 22–25 weeks of pregnancy.
Based on all the data, the geneticist will be able to give an opinion about the development of your child.
Ultrasound at the 12th week of pregnancy: heart rate 165; ktr 54; TVP 1.6 mm, nasal bones are visible
Free hCG 26.49/0.490 MoM; PAPP-A 4.162/1.091 MoM
Trisomy 21 - basic risk 1:734, individual risk 1:14683
Trisomy I18 - basic risk 1: 1707, individual risk<1:20000
Trisomy 13-basic risk 1:5376, individual risk<1:20000
Hello. Please help me decipher the results of biochemical screening of the 1st trimester. They said that I was in a risk group, I’m very worried. Age 33 years, height 166, weight 51 kg
According to ultrasound, the period is 12 weeks.5 days.
KTR 63.1, TVP 1.6, PI- 1.23, BPR - 18.4, OG- 70, coolant - 55, DB -7.8, DNA-2.3 mm, BZ-2.0 mm, ultrasonic markers No chromosomal diseases were identified.
Biochemical screening: heart rate - 156, CTE - 63.1, TVP - 1.60, nasal bone is determined by PIVP 1.23
HCG 265.00 IU/l /6.953 MoM
PAPP-A 4.140 IU/l / 1.164 MoM
Trisomy 21 base risk 1:389, ind. risk 1:154
Trisomy 18 base risk 1:946, ind. risk 1:18928
Trisomy 13 base risk 1:2970, ind. risk 1:59399
Hello. Please help me understand the first screening. I am 34 years old, weight 93. Neither I nor my husband had any abnormalities in our family. The first day of the last menstruation was 08/06/17. When registering, type 2 diabetes was detected. In the first days I also take Duphaston and Utrozhestan, because the threat of miscarriage remains. Here is the result of the ultrasound. Pregnancy week. KTR - 49 mm, heartbeat is determined, heart rate - 176 beats / min. The yolk sac is visualized - 5 mm. TVP - 1.1 .nasal bone 2.2.bpr-16 mm.lzr-20 mm.olzh-52 mm.hip-4.8 mm.shoulder-4.3 mm.fetal anatomy: butterfly+.spine +.stomach+.anterior abdominal wall+.bones cranial vault +. bladder +. limbs +. predominant localization of the chorion: posterior wall of the uterus. thickness - 12 mm. chorion structure: unchanged. dshm 58 mm. vmz closed. blood test. holy beta subunit hCG - 14.02 IU/l/ 0.231 MoM.papp_a-0.651IU/l/ 0.142 MoM..
Trisomy 21 basic 1:271, individual 1:1261.
Trisomy 18 1:612, individual 1:33.
Trisomy. 13 1:1933, individual 1:174. Thanks in advance for your answer.
Help me understand the screening conclusion: according to biopsy, Down syndrome is 1:155, hcgb -ng/ml 105.0 normal MOM 2.20, Papp-a -mm -3981.80 - normal MOM 1.17, pigf- 21.9 MOM 0.53 , nc - 1.7 mm, tvp - 1.2 mm, ktr - 60 mm, bpr - 20.7, og - 73 mm, cool - 63 cm, vpr normal, sb rhythm correct, down syndrome: low risk, 1 :10207 not biopsy
Screening was carried out a week ago, I am 31 years old
Good afternoon Help me understand the conclusion of 1 screening. Screening was carried out at 12 weeks 1 day.
Ultrasound - period 12 weeks + 1 days according to KTR
Fetal heart rate bpm
hCG - 68.70 IU/n/1.661 MoM
PAPP-A - 5.118 IU/n/1.638 MoM
For GI doctors: an individual risk of 1:101 and above (1:102, 1:103...) is considered low
trisomy 21 - base risk - 1:595, ind. risk 1:11895
trisomy 18 - base risk - 1:1397, ind. risk 1:20000
trisomy 13 - base risk - 1:4397, ind. risk 1:20000
I forgot to indicate the age - 30 years old, the anemnesis shows 2 frozen pregnancies at 7 weeks.
Good afternoon Today I had my first screening. Help me to understand. Duration 12 weeks. I am 32 years old, this is my second pregnancy, the first went well, I gave birth to a healthy baby 2 years ago. There are no children with disabilities or syndromes in my family. The ultrasound said that everything was normal, but the blood results were not very good and the doctor called them scissors. Indicators:
Chorion high on the anterior wall
Umbilical cord 3 vessels
The nasal bone is determined; Doppler measurements of the tricuspid valve are normal.
There are no sizes of the fruit, only a description:
Head/brain looks normal
The spine looks normal
Heart 4-chamber section normal
The belly looks normal
Bladder/kidneys identified
Arms, legs: identified, both visible
Trisomy 21: baseline 1:447; individual (basic+ultrasound+BC) 1:1770
Trisomy 18: baseline 1:1033; individual (basic+ultrasound+BC) 1:20652
Trisomy 13: baseline 1:3255; individual (basic+ultrasound+BC) 1:65092
It seems that all the indicators are normal, but I am concerned about the blood results (biochemistry of maternal serum):
hCG: 120.65 IU/l/2.807 MoM
PAPP-A: 0.584 IU/l/0.496 MoM
Tell me how great the risk of pathology is and should I worry, otherwise I’ve already exhausted myself.
You still have the following questions:
- Your weight.
- Your height.
- Do you have any concomitant diseases: diabetes mellitus, thyroid pathology, hypertension and others.
- Are you taking any medications?
- How is the pregnancy progressing: is there any toxicosis or signs of miscarriage, including pain in the lower abdomen or discharge from the genital tract.
At 12 weeks of pregnancy, the following indicators are considered the norms for ultrasound screening:
- Fetal heart rate - 150–174 beats per minute;
- KTR - 51–59 mm;
- TVP - 1.6–2.5 mm;
- BPR - 20 mm;
- chorion - located high above the internal os along the anterior or posterior wall or in the fundus of the uterus;
- umbilical cord - has 3 vessels;
- nasal bones - clearly visualized, more than 3 mm;
- internal organs - without features.
Based on the results of biochemical screening, the following indicators are considered normal:
- free beta-hCG subunit and PAPPA-A - from 0.5 to 2.0 MoM;
- risks for all indicators are more than 1:380.
In your case, there is an increase in beta-hCG, which may indicate:
- Down syndrome;
- multiple pregnancy;
- severe toxicosis;
- diabetes mellitus in the mother.
An increase in beta-hCG levels can be caused by:
- undergo a second biochemical screening at 16–20 weeks of pregnancy;
- If indicated, consult a geneticist.
1. Miscarriages occurred at 7 and 9 weeks.
2. The reasons were not established.
3. There was no examination, but before the real pregnancy (immediately after the miscarriage I took Regulon for 3 months, after the withdrawal I immediately became pregnant unplanned)
4.Spouse’s age is 45 years.
5. There were no allocations, but for screening I traveled 100 km by bus, then walked about 1 km, since I had never been to the regional center before, I was looking for a residential complex. Maybe something was overextended there.
6. My gynecologist didn’t refer me to a geneticist right away; she said that she would send me after the second screening.
7. The geneticist explained the risks, I refused cordocentesis, and as a result, analysis after the birth of the child for CA is all that remains.
8. Ultrasound 1 screening CTE 62, HR 160, TVP 1.8 nasal bridge length 2.2 Echofocus in the left ventricle MHA-golf ball. Duration 12 weeks 6 days.
Ultrasound 2 screening BDP 53, fronto-occipital size 69, left femur 34, tibia 30, humerus 32, forearm 29, head circumference 190 mm, abdominal diameter 50, right femur 34, right tibia 30, right humerus 32, forearm 29. The anatomy of the fetus is completely unremarkable. Features: echofocus in the left ventricle.
9. On the second biochemical. screening at 17 weeks (done in our laboratory, I was then in the hospital with increased tone, tested 2 days before discharge right in the hospital) AFP 73.7 IU per ml, hCGmme per ml. Utrozhestan was 200 mg per day.
10. No correction was made for Utrozhestan.
If an ultrasound does not detect a golf ball at 32 weeks, does this mean that there is no diabetes or is it just an analysis after birth?
Thanks for the additions to your question.
Based on all the data you provided, I can draw the following conclusions.
You needed to schedule a genetic consultation no later than 18–20 weeks of pregnancy, taking into account:
- the presence of two spontaneous miscarriages in the early stages;
- lack of examination after miscarriages;
- your age - 35 years old;
- your husband’s age is 45 years;
- the presence of risks of having a child with a chromosomal abnormality based on the results of ultrasound and biochemical studies;
- the presence of an ultrasound marker of a chromosomal abnormality in the fetus.
If you were to see a geneticist, additional invasive testing might be possible.
To determine your child's condition, you needed to undergo cordocentesis suggested by a geneticist. There are risks of miscarriage after the procedure, however, only an invasive study would give you the answer to all your questions.
The condition of the child and the presence of a chromosomal abnormality can be judged only after the results of the examination. In your case, it is necessary to check the child after birth for CA.
An ultrasound examination allows one to identify the risks of developing a particular pathology in the fetus, without making a diagnosis. Additional more precise research is needed.
Hello Irina, explain my screening. I am 42 years old, third pregnancy, third birth, type 2 diabetes mellitus, 12 weeks and five days. Heart rate 169; CTE 63; TVP 2.00 mm; nasal bone determined; Doppler ductus venosus 1.00; hCG 28.87IU/l /1.100MoM;PPAP-2.281IU/l /1.116MoM
Trisomy 21 basic 1:43 ind1:864
Trisomy 18. basic 1:105 ind1:2101
Trisomy 13 basic 1:330 ind1:6594
Hello Irina Vyacheslavovna. Help me decipher my first screening.
I am 38 years old. Term 12 weeks + 5 days according to KTR.
Fetal heart rate 158 beats/min
The nasal bone is identified.
Free beta subunit of hCG -17.47 IU/l/0.528 MoM
PAPP-A 2.129 IU/l/ 0.719 MoM
Trisomy 21 Basic 1:109 Individual 1:2177
Trisomy 18 Basic 1:265 Individual 1:5295
Trisomy 13 Basic 1:831 Individual 1:16618
Please help me, I can’t find a place for myself, I’m very worried.
Irina, good afternoon!
I am 28 years old, period 12.1 (due at the time of ultrasound)
Fetal heart rate 164 beats/min
Life Cycle program PTO PAPP-A - 0.89; Free hCGB - 2.78
Astraia program PTO PAPP-A - 0.98; Free hCGB - 3.38
Down syndrome 1:1718 (Life Cycle program), 1:10667 (Astraia program)
Edwards syndrome 1:(Life Cycle program), 1:35817 (Astraia program)
Patau syndrome 1:(Life Cycle program), 1:(Astraia program)
Turner Syndrome 1:(Life Cycle Program)
Triploily 1:(Life Cycle program)
Thank you very much in advance.
Irina, good afternoon!
Please help me decipher the results of the first screening.
I am 30 years old, period 12.1 (due at the time of ultrasound)
weight - 63kg, height 162cm
First pregnancy, there were no anomalies on my side or my husband’s side
Fetal heart rate 162 beats/min
Interparietal (BPR) - 20.0mm
Chorion/placenta - low on the anterior wall
amniotic fluid - normal amount
umbilical cord - 3 vessels
head/brain - looks normal, spine looks normal, anterior abdominal wall looks normal, stomach is visible, bladder/kidneys are visible, both arms/legs are visible.
free hCG beta subunit 21.9 IU/l equivalent to 0.595 MoM
PAPP-A - 6.182 IU/L equivalent to 2.544 MoM
Trisomy 21 basic risk 1:573 /individual 1:11451
Trisomy 18 base risk 1:1366< 1:20000
Trisomy 13 base risk 1:4293< 1:20000
Thank you very much in advance.
Hello! please help me understand the test results.
pregnancy at the time of testing 12+5 days
there was no one on the family line with deviations or defects.
second pregnancy (first without pathologies) child 10 years old
hCG 17.32 IU/l /0.571 MoM
PAPP-A 2.283IU/L /1.141MoM
trisomy 21 individual 1:777, basic 1:15536
trisomy 18 individual 1:898 basic 1:37967
trisomy 13 individual 1: 5955 basic 1: 119098
Please tell me if there is a risk of having a child with pathology based on the results of these tests.
Hello, please help me figure this out.
Screening 12 days and 4 days
Weight: 62.45 Height: 165 Age: 35. First day of menstruation: 09.25.2017
Nasal bone: determined; Tricupsidal valve Doppler: normal; Tricupsidal valve Doppler: normal; Dopplerometry of the venous duct: 0.80;
Free hCG beta subunit: 104.00 IU/l / 2.003MoM
PAPP-A 0.696IU/l / 0.313MoM
Trisomy 21: basic (1:245) individual (1:1265)
Trisomy 18: basic (1:587) individual (1:11743)
Trisomy 13: basic (1:1845) individual (1:18268)
The doctor referred me to a geneticist. What's wrong?
Hello, please help me figure it out!
Screening 1st trimester
term under DPM -12 weeks + 0 days.
term according to KTR - 12 weeks + 3 days.
age - 42, height 160 cm, weight 77.2, pregnancy -1 (natural)
Smoking, diabetes, heredity - no
visualization - fetal position limited
The nasal bone is determined
B - hCG - 33.68 IU/l - equivalent 0.898 MoM
PPAP-A - 2.341 IU/l equivalent to 1.101 MoM
Risks Basic Individual
Trisomy 21 1:44 1:890
Trisomy18 1:107 1:2139
Trisomy 13 1:336 1:6721
The ultrasound specialist said everything was fine, the doctor didn’t say anything...
Did I read your article and was worried about something? I'm completely confused about the risks!
Thank you for your reply
Hello, I'm 24. Ultrasound 12 over. 6 to.
VN+, NK+, hands+, feet+, butterfly+, urinary+, stomach+ on+, HF+, LF+
Komircevy space 1.6 mm, nasal bone 3.4 mm
Heart rate 156 bpm
Motor activity is normal
Corresponds to 12 over. 6 days Low placentation
Free b-hCG 0.380 mOhm
Rarr-a 1.330 mOhm
Initial risk 21 1:988, 18 1:2446, 13 1:7665
Revised risk 21 1:7048, 18 1:17451, 13 1:54678
The geneticist said there are abnormalities, you need to donate blood within a week
Hello, help me figure it out! 25 years old, ultrasound 13 weeks + 2 days according to Ktr. HR 154, CTE 71.0; TVP 1.70; pl 1.01; hCG 13.60;\ 0.362 mom. papp-a 0.998; \0.644 mom
trisomy 21 base 1:964(individual 1:19274) trisomy 18 base 1:2432(individual<1:20000) трисомия 13 базовый 1:7607 (индивид <1:20000)
Hello! Help me figure out the free beta subunit of hCG 1.379MoM, PAPP-A 0.695; trisomy 21 basic 1:887, individual. 1:9064, 18 base trisomy. 1:2137 individual<1:20000, трисомия 13 баз. 1:6712 индивид. <1:20000
Hello! Tell me the risk of developing Down syndrome. Screening 1 indicators are as follows
the nasal bone is visualized
no tricuspid regurgitation was detected
orthrograde blood flow PI 0.91
hCGb 177.3 mom 3.55
papp-a 3430.2 mom 1.14
Hello. Today we did screening for 12 weeks, according to the protocol the indicators are: ktr - 51.7 heart rate - 159, tvp - 1.2 nasal bone - 1.5 bpr - 13.8 - 11.6. I'm worried about TVP and BPR.
Good afternoon, according to the results of the first screening, the ultrasound conclusion was that there were no suspicions of congenital birth defects, but the serum indicators were as follows (gestational age 12 weeks)
free hCG beta subunit: 12.9 IU/l / 0.298 MoM
APP-A: 1.180IU/l / 0.389 MoM
Trisomy 21 basic risk 1:936 individual 1:18727
Trisomy 18 bases. risk 1:2244 individual 1:1550
Trisomy 13 base risk 1:7052 individual 1:20000
The doctor did not give any explanations; they sent me for the 2nd screening at 20 weeks.
After the second screening, the doctor’s conclusion is as follows: “The abdominal section of the umbilical vein has a right-sided course, the gallbladder is located to the left of the umbilical vein, the right umbilical vein is persistent.”
We scheduled a consultation with geneticists, but in our city they are by appointment only. I made an appointment, but the wait is still long. Already all exhausted. I don't know what to think. The doctor again did not give any explanation. Help me figure it out, please
Krutieva Natalya Nikolaevna
Povarova Maria Viktorovna
ENT doctor (otorhinolaryngologist, otolaryngologist)
Suyurova Aliya Rafikovna
Ultrasound doctor
Reviews
License No. LO791 dated January 24, 2017
Center for Immunology and Reproduction © CIR Laboratories LLC 2006–2017
Ultrasound during pregnancy at 12 weeks
Every pregnant woman is required to undergo an ultrasound examination of her unborn child (fetus) at 12 weeks of pregnancy. Ultrasound at this stage is screening. Deciphering this study is quite difficult. The results obtained during an ultrasound scan at week 12 are the most informative for an obstetrician-gynecologist.
If you haven’t had an ultrasound yet at an early stage, then 12 weeks is the most appropriate time to do it. In general, the first mandatory study can be done at 11, 13, and 14 weeks, but most women are still sent for it at 12 weeks.
A woman’s uterus is already enlarged by more than 2 times its original size. It is about 10 cm in diameter, and its bottom (that is, the uppermost part) is approximately level with the pubic bones. It does not yet extend beyond the pelvis into the abdominal cavity, so trying to palpate it through the abdomen is useless. But it is already large enough for an ultrasound to be done without using a vaginal probe. Typically, the examination is performed in the classical way, through the skin of the abdomen.
An ultrasound performed at 12 weeks is not only not harmful, but also useful - in the sense that it allows you to find out information that is not available to research done at other times (before 11 and after 14 weeks).
It is at this time that it is possible to make the first assumption that the child may have some kind of disorder. Based on this, the main purpose of an ultrasound at 12 weeks is not even to determine pregnancy or anything else, but to identify developmental defects. Although, of course, all other available indicators are also determined during this procedure.
What is important during an ultrasound at 12 weeks of pregnancy?
During an ultrasound scan of the fetus at 12 weeks of pregnancy, a number of very important measurements are taken to identify the risk group for chromosomal abnormalities of the fetus. It has been established that the most optimal period for screening in the first trimester of pregnancy is 12 weeks of pregnancy (from 11 to 13 weeks and 6 days). During an ultrasound of the fetus at 12 weeks of pregnancy, in addition to the length of the embryo (coccygeal-parietal size - CTR), the size of the fetal head (head circumference, biparietal size, fronto-occipital size) is measured. An assessment of the structures of the fetal brain and the symmetry of the hemispheres is mandatory during an ultrasound scan of the fetus at 12 weeks of pregnancy. Normally, the fetal brain looks like a butterfly on ultrasound. The long bones of the fetus are measured (humerus, ulna, radius, femur, tibia, fibula), and the symmetry of the limbs and their motor activity are assessed. During an ultrasound of the fetus at 12 weeks of pregnancy, the transverse size of the fetal abdomen, abdominal circumference are measured, and the presence of the stomach and heart in typical places is noted. When performing an ultrasound of the fetus at 12 weeks of pregnancy, the presence of heart defects can be suspected if the resolution of the ultrasound scanner is sufficient and the ultrasound operator is properly experienced and educated. There are published data on the diagnosis of transposition of the great vessels, common atrioventricular canal, ectopia of the heart, etc., recorded during fetal ultrasound at 12 weeks of pregnancy.
The main thing that interests a specialist when performing an ultrasound is, of course, the fetus. Its size during this period is comparable to the length of a woman’s little finger, the heart rate is up to 160 beats per minute, the yolk sac is no longer visualized, the developing placenta can be attached to any of the walls or bottom of the uterus.
The doctor not only sees the very outlines of the child, but also examines his organs, accessible visualizations: the bones of the cranial vault, stomach, anterior abdominal wall, bladder, nose, spine, bones of the limbs. The size of the nasal bones and collar area is also assessed; changes in these areas may indicate that the child may have chromosomal abnormalities. At week 12, the thickness of the collar space is 1.5-1.8 mm, the size of the nasal bones is 1.6-1.9 mm.
During an ultrasound examination at 12 weeks, specialists working with good machines can sometimes make an assumption about the sex of the child, but this assumption is not always accurate, so you should not rely on it.
What does a baby look like at 2 weeks of pregnancy?
The size of the child from the crown to the tailbone is about 5-6 cm, which is already quite large compared to what it was exactly half the term ago, when the size of the embryo was only 5-6 mm. During this period, the child is actively growing, when examined, one can see him as a very cute little man with short arms and legs, which causes tenderness in expectant mothers, and even tears in the most sensitive of them. The child moves actively, waves his arms, kicks his legs, and yawns.
All the main organs have already been laid, now the baby just has to wait until they mature and develop to their full potential. Even the placenta, in general, is already formed, although, of course, it is still very far from final maturity. However, this does not mean that in all subsequent weeks the child will “rest”, simply grow and gain weight; in fact, development processes are ongoing and will continue to be in full swing. At 12 weeks, the baby's intestines begin to peristalt for the first time, he acquires fingerprints, his kidneys begin to function, and so on.
Possible pathologies on ultrasound at 12 weeks of pregnancy
The main task of ultrasound is to determine developmental defects. If an abnormality is suspected, the patient is sent to a geneticist, who determines the likelihood of having a child with problems. If this probability is high, the woman is offered a difficult decision - to terminate the pregnancy or keep the child.
In addition to defects, ultrasound detects such disorders as signs of underdevelopment of the baby, low attachment of the placenta, hypertonicity of the uterus and much more. All identified disorders must be recorded in the conclusion to the procedure. Then the gynecologist studies the research protocol and, based on his findings, offers the expectant mother one or another treatment option.
An ultrasound at 12 weeks of pregnancy measures the following indicators:
The ovum is defined as a rounded anechoic formation, which is surrounded by a thin rim, an area of increased echogenicity. Most often localized in the upper third of the uterine cavity. To determine the average internal diameter of the fetal egg, its length and anteroposterior size are measured during sagittal scanning, as well as its transverse size during transverse scanning. After these measurements, the arithmetic mean of these three sizes is calculated. Measurements are taken along the internal contour of the fertilized egg.
The average internal diameter of the ovum is a fairly variable value and the error in determining the gestational age using this indicator can reach 1.5 weeks. If there is no image of the embryo in the fertilized egg and its average internal size is more than 16 mm, it is assumed that there is a non-developing pregnancy of the anembryonic type.
This diagnosis is finally confirmed by a control ultrasound examination.
The yolk sac is practically undetectable by the end of the 12th week, since during this period the placenta begins to synthesize progesterone in sufficient quantities.
Measurement of fetal fetometric parameters and heart rate can be used for early detection of pregnancy pathology. Normally, a baby's heart rate at 12 weeks is between 110 and 170 beats per minute. The weight of the fetus at this stage is 8-15 grams and has a sedentary position. It is impossible to determine the sex of the unborn child at 12 weeks of pregnancy.
Ultrasound results help to identify unfavorable prognostic signs in the early stages of pregnancy up to 12 weeks:
The results obtained will help identify major malformations, such as anencephaly and space-occupying defects of the anterior abdominal wall.
Coccygeal-parietal size of the fetus.
Using ultrasound, the coccygeal-parietal size (CPR) of the fetus (child) is measured, which is the most accurate parameter for determining the gestational age. The coccygeal-parietal size at 12 weeks is 53 mm, which is normal. If there is a slight deviation, there is no reason to worry, since small normal fluctuations are possible, which on average will range from 42 to 59 mm.
Biparietal diameter (BPD) of the head
By the end of the 12th week, as an additional indicator for determining the gestational age, the biparietal diameter (BPD) of the embryo's head is also measured. Standard indicators. The confidence interval for determining the measured parameters on ultrasound is ±6 days for CTE, as well as ±8 days for BPD.
Determining the thickness of the collar space
In recent years, ultrasound determination of the thickness of the nuchal translucency at 12 weeks of pregnancy has become a fairly important sign that allows one to suspect chromosomal abnormalities, especially trisomy 21. This is a transient symptom, usually detected only between the 11th (±0 days) and 13th (±6 days) weeks of pregnancy. Both abdominal and transvaginal examinations can detect this sign in the mediosagittal plane of scanning of the embryo or fetus.
The thickness of the collar space is determined from the inner edge of the skin to the soft tissue of the back of the head. A thickness of 3 mm or more is a generally accepted pathological sign. The amniotic membrane, in the absence of its fusion with the chorion membrane, can sometimes imitate the nuchal space.
The risk of chromosomal abnormalities increases markedly with increasing nuchal translucency thickness. Therefore, whenever the nuchal translucency thickness is 3 mm or more, karyotyping using chorionic villus sampling or early amniocentesis is necessary. For young women under 35 years of age who do not have increased risk factors for chromosomal abnormalities, non-invasive screening ultrasound may be recommended.
Threat of miscarriage during ultrasound
The threat of miscarriage during ultrasound is usually assessed by two signs - local thickening of the myometrium and the presence of retrochorial hematoma. Local thickening of the uterine wall is a manifestation of hypertonicity of the myometrial area and looks like an increase in the thickness of the uterine wall without clear boundaries with bulging of the internal contour towards the fertilized egg.
The shape of the fertilized egg can vary from round to oval, flattened or irregular. Detection of short-term local myometrial tone without clinical signs of threatened miscarriage is considered as a normal variant and should not serve as a basis for prescribing maintenance therapy.
Trophoblastic disease
Long-term hypertonicity of the myometrium is an indicator of chorion detachment and impaired trophoblast invasion.
Trophoblastic disease. With the development of this complication, the following features of the ultrasound picture are revealed - the size of the uterus exceeds the normative values for the duration of pregnancy, the uterine cavity is expanded and filled with anechoic structures of various sizes and shapes, as well as structures of increased echogenicity of irregular shape. At the same time, on ultrasound you can see that not the entire fertilized egg may be involved in the process, but only part of it. An additional sign of trophoblastic disease on ultrasound is the detection of thecallutein ovarian cysts, but usually by the end of the 12th week they are practically no longer detectable.
First trimester prenatal screening
In addition to the measurements listed above, when performing an ultrasound of the fetus at 12 weeks of pregnancy, screening for chromosomal pathologies of the fetus is carried out. It has been established that most chromosomal pathologies are accompanied by an increase in the nuchal space located in the fetal neck. This feature is caused by the fact that with chromosomal abnormalities of the fetus, in particular with Down syndrome, the skin has increased folding, i.e., roughly speaking, there is more skin. Fluid accumulates under such skin, which contributes to the visualization of thickening of the collar zone during ultrasound of the fetus at 12 weeks of pregnancy. In fetuses with a karyotype disorder (due to chromosomal diseases), the thickness of the nuchal zone is 2.5 mm (or more) greater than the average value for a given period of pregnancy in fetuses with a normal karyotype.
Ultrasound of the fetus at 12 weeks of pregnancy with Down syndrome
In addition to the enlarged nuchal region in trisomy 21 (Down syndrome), 60–70% of fetuses have no visible nasal bones. It is noticed that people with Down syndrome have a short nose. During embryogenesis, the nose in Down syndrome (nasal bones) is formed later than in fetuses with a normal karyotype. Also, from 15 to 21 weeks of pregnancy, there is an increased incidence of shortening of the nasal bones compared to the average values for this period of pregnancy in fetuses with Down syndrome.
In fetuses with Down syndrome, there is a shortening of the upper jaw, which results in smoothness of the contours of the face.
In fetuses with Down syndrome, Doppler measurements determine the pathological nature of the blood flow velocity curves in the ductus venosus. Assessment of the nature of blood flow in the venous duct is one of the mandatory screening parameters when performing fetal ultrasound at 12 weeks as part of prenatal screening in the first trimester. Reverse blood flow in the ductus venosus is considered pathological.
Ultrasound of the fetus at 12 weeks of pregnancy with Edwards syndrome
Trisomy 18 (Edwards syndrome) is characterized by early manifestations of slow fetal development and a tendency to bradycardia (decreased fetal heartbeat). Moreover, until a certain stage of pregnancy, the fetus develops normally (usually up to 8 weeks of pregnancy)
In fetuses with Edwards syndrome, an omphalocele is detected (a hernia of the abdominal cavity with displacement of the abdominal organs into the hernial sac).
In fetuses with Edwards syndrome, there is a lack of visualization of the nasal bones.
In fetuses with Edwards syndrome, a single umbilical cord artery is a common finding. Normally, the umbilical cord has two arteries and one vein.
Ultrasound of the fetus at 12 weeks of pregnancy with Patau syndrome
With trisomy 13, 70% of fetuses experience tachycardia (increased heart rate).
Also, in fetuses with Patau syndrome, early detection of fetal growth retardation may occur.
Fetuses with Patau syndrome have megacystis (enlarged bladder).
Holoprosencephaly in fetuses with Patau syndrome (a disorder of brain formation) and omphalocele are often combined signs detected by ultrasound of the fetus at 12 weeks of pregnancy.
Ultrasound of the fetus at 12 weeks of pregnancy with Turner syndrome
With Turner syndrome, 50% of fetuses experience tachycardia (rapid heart rate of more than 160 beats per minute) and early manifestations of slow fetal development (the size of the fetus no longer corresponds to the gestational age, usually from the 8th week of pregnancy. Ultrasound of the fetus at 12 weeks of pregnancy with Triploidy syndrome
Triploidy is characterized by early signs of slower development of the asymmetric type.
Bradycardia (heart rate below 120 beats per minute), holoprosencephaly (impaired division of the brain into sections, and, accordingly, the impossibility of normal mental development of the child), omphalocele (eversion of the abdominal organs into the hernial sac in the umbilical cord area) are also characteristic of triploidy.
Posterior fossa cysts, choroid plexus cysts. Cysts are accumulations of fluid in the brain. The presence of bilateral cysts is considered an unfavorable sign, while the isolated presence of one small cyst in the brain (in particular, choroid plexus cysts) and the absence of other markers of chromosomal diseases are not regarded as a pathology and require dynamic monitoring.
Early pyelectasis (enlargement of the renal pelvis) is also a marker of chromosomal pathologies of the fetus.
All this data can be recorded during an ultrasound scan of the fetus at 12 weeks of pregnancy. It is important to note that the presence of these markers is not a diagnosis that reliably confirms the presence of chromosomal pathology in the fetus. If several of the above markers of fetal chromosomal pathologies are detected during ultrasound, invasive prenatal diagnosis is recommended to obtain material of fetal origin. These procedures include amniocentesis and chorionic villus sampling. After obtaining a section of chorion (placenta) or amniotic fluid, the child’s chromosome set is determined (karyotyping). Only karyotyping is the basis for diagnosing a chromosomal abnormality in the fetus.
Screening in the first trimester of pregnancy - what you need to know about the norms and results
Almost every pregnant woman has heard something about screening in the first trimester of pregnancy (prenatal screening). But often even those who have already completed it do not know what exactly it is prescribed for.
And for expectant mothers who are yet to do this, this phrase sometimes seems frightening. And it scares only because the woman does not know how this is done, how to interpret the results obtained later, and why the doctor needs this. You will find answers to these and many other questions related to this topic in this article.
So, more than once I had to deal with the fact that a woman, having heard the incomprehensible and unfamiliar word screening, began to draw terrible pictures in her head that frightened her, making her want to refuse to undergo this procedure. Therefore, the first thing we will tell you is what the word “screening” means.
Screening (English screening - sorting) are various research methods, which, due to their simplicity, safety and accessibility, can be used en masse in large groups of people to identify a number of signs. Prenatal means prenatal. Thus, we can give the following definition to the concept of “prenatal screening”.
Screening in the first trimester of pregnancy is a set of diagnostic tests used in pregnant women at a certain stage of pregnancy to identify gross malformations of the fetus, as well as the presence or absence of indirect signs of pathologies of fetal development or genetic abnormalities.
The acceptable period for screening in the 1st trimester is 11 weeks - 13 weeks and 6 days (see the calculator for calculating the gestational age by week). Screening is not carried out earlier or later, since in this case the results obtained will not be informative and reliable. The most optimal period is considered to be the obstetric weeks of pregnancy.
Who is referred for first trimester screening?
According to Order No. 457 of the Ministry of Health of the Russian Federation of 2000, prenatal screening is recommended for all women. A woman can refuse it, no one will force her to do this research, but doing this is extremely reckless and only speaks of the woman’s illiteracy and negligent attitude towards herself and, above all, towards her child.
Risk groups for whom prenatal screening should be mandatory:
- Women whose age is 35 years or more.
- The presence of a threat of termination of pregnancy in the early stages.
- History of spontaneous miscarriage(s).
- History of missed or regressed pregnancy(es).
- Presence of occupational hazards.
- Previously diagnosed chromosomal abnormalities and (or) malformations in the fetus based on screening results in past pregnancies, or the presence of children born with such anomalies.
- Women who have had an infectious disease in early pregnancy.
- Women who took medications prohibited for pregnant women in the early stages of pregnancy.
- Presence of alcoholism, drug addiction.
- Hereditary diseases in the family of a woman or in the family of the child’s father.
- I have a close relationship between the mother and father of a child.
Prenatal screening during the weeks of pregnancy consists of two research methods - ultrasound screening of the 1st trimester and biochemical screening.
Ultrasound examination as part of screening
Preparation for the study: If the ultrasound is performed transvaginally (the sensor is inserted into the vagina), then no special preparation is required. If the ultrasound is performed transabdominally (the sensor is in contact with the anterior abdominal wall), then the study is carried out with a full bladder. To do this, it is recommended not to urinate 3-4 hours before the test, or drink 1 ml of still water an hour and a half before the test.
Necessary conditions for obtaining reliable ultrasound data. According to the norms, screening of the first trimester in the form of ultrasound is carried out:
- No earlier than 11 obstetric weeks and no later than 13 weeks and 6 days.
- The CTP (coccygeal-parietal size) of the fetus is not less than 45 mm.
- The position of the child should allow the doctor to adequately take all measurements; otherwise, it is necessary to cough, move, walk for a while so that the fetus changes its position.
As a result of ultrasound, the following indicators are examined:
- CTP (coccygeal-parietal size) – measured from the parietal bone to the coccyx
- Head circumference
- BDP (biparietal size) - the distance between the parietal tuberosities
- Distance from frontal bone to occipital bone
- Symmetry of the cerebral hemispheres and its structure
- TVP (collar thickness)
- Fetal heart rate (heart rate)
- Length of humerus, femur, forearm and shin bones
- Location of the heart and stomach in the fetus
- Sizes of the heart and great vessels
- Placenta location and thickness
- Water quantity
- Number of vessels in the umbilical cord
- Condition of the internal os of the cervix
- Presence or absence of uterine hypertonicity
Decoding of the received data:
What pathologies can be detected by ultrasound?
Based on the results of ultrasound screening in the 1st trimester, we can talk about the absence or presence of the following anomalies:
- Down syndrome is trisomy 21, the most common genetic disorder. The prevalence of detection is 1:700 cases. Thanks to prenatal screening, the birth rate of children with Down syndrome has decreased to 1:1100 cases.
- Pathologies of neural tube development (meningocele, meningomyelocele, encephalocele and others).
- Omphalocele is a pathology in which part of the internal organs is located under the skin of the anterior abdominal wall in the hernial sac.
- Patau syndrome is trisomy on chromosome 13. The incidence is on average 1:10,000 cases. 95% of children born with this syndrome die within a few months due to severe damage to internal organs. Ultrasound shows increased fetal heart rate, impaired brain development, omphalocele, and delayed development of tubular bones.
- Edwards syndrome is trisomy on chromosome 18. The incidence rate is 1:7000 cases. It is more common in children whose mothers are over 35 years old. An ultrasound shows a decrease in the fetal heartbeat, an omphalocele, the nasal bones are not visible, and one umbilical artery instead of two.
- Triploidy is a genetic abnormality in which there is a triple set of chromosomes instead of a double set. Accompanied by multiple developmental defects in the fetus.
- Cornelia de Lange syndrome is a genetic anomaly in which the fetus experiences various developmental defects, and in the future, mental retardation. The incidence rate is 1:10,000 cases.
- Smith-Opitz syndrome is an autosomal recessive genetic disease manifested by metabolic disorders. As a result, the child experiences multiple pathologies, mental retardation, autism and other symptoms. The average incidence is 1:30,000 cases.
Learn more about diagnosing Down syndrome
Mainly, ultrasound examination during the weeks of pregnancy is carried out to detect Down syndrome. The main indicator for diagnosis becomes:
- Neck space thickness (TNT). TVP is the distance between the soft tissues of the neck and the skin. An increase in the thickness of the nuchal translucency may indicate not only an increased risk of having a child with Down syndrome, but also that other genetic pathologies in the fetus are possible.
- In children with Down syndrome, the nasal bone is most often not visualized for a period of weeks. The contours of the face are smoothed.
Before 11 weeks of pregnancy, the thickness of the nuchal translucency is so small that it is impossible to adequately and reliably assess it. After the 14th week, the fetus develops a lymphatic system and this space can normally be filled with lymph, so the measurement is also not reliable. The incidence of chromosomal abnormalities in the fetus depending on the thickness of the nuchal translucency.
When deciphering the screening data of the 1st trimester, it should be remembered that the thickness of the nuchal translucency alone is not a guide to action and does not indicate a 100% probability of the presence of the disease in the child.
Therefore, the next stage of screening of the 1st trimester is carried out - taking blood to determine the level of β-hCG and PAPP-A. Based on the obtained indicators, the risk of having a chromosomal pathology is calculated. If the risk based on the results of these studies is high, then amniocentesis is suggested. This is taking amniotic fluid for a more accurate diagnosis.
In particularly difficult cases, cordocentesis may be required - taking cord blood for analysis. Chorionic villus sampling may also be used. All of these methods are invasive and carry risks for the mother and fetus. Therefore, the decision to perform them is decided by the woman and her doctor jointly, taking into account all the risks of carrying out and refusing the procedure.
Biochemical screening of the first trimester of pregnancy
This stage of the study must be carried out after an ultrasound scan. This is an important condition, because all biochemical indicators depend on the duration of pregnancy, down to the day. Every day the norms of indicators change. And ultrasound allows you to determine the gestational age with the accuracy that is necessary for conducting a correct study. At the time of donating blood, you should already have ultrasound results with the indicated gestational age based on CTE. Also, an ultrasound may reveal a frozen pregnancy or a regressing pregnancy, in which case further examination does not make sense.
Preparing for the study
Blood is drawn on an empty stomach! It is not advisable to even drink water in the morning of this day. If the test is carried out too late, you are allowed to drink some water. It is better to take food with you and have a snack immediately after blood sampling rather than violate this condition.
2 days before the scheduled day of the study, you should exclude from your diet all foods that are strong allergens, even if you have never been allergic to them - these are chocolate, nuts, seafood, as well as very fatty foods and smoked foods.
Otherwise, the risk of obtaining unreliable results increases significantly.
Let's consider what deviations from normal levels of β-hCG and PAPP-A may indicate.
β-hCG – human chorionic gonadotropin
This hormone is produced by the chorion (“shell” of the fetus), thanks to this hormone it is possible to determine the presence of pregnancy in the early stages. The level of β-hCG gradually increases in the first months of pregnancy, its maximum level is observed during the weeks of pregnancy. Then the level of β-hCG gradually decreases, remaining unchanged throughout the second half of pregnancy.
- Down syndrome
- Multiple pregnancy
- Severe toxicosis
- Maternal diabetes mellitus
- Edwards syndrome
- Ectopic pregnancy (but this is usually established before biochemical testing)
- Placental insufficiency
- High risk of miscarriage
PAPP-A – pregnancy associated protein-A
This is a protein produced by the placenta in the body of a pregnant woman, responsible for the immune response during pregnancy, and is also responsible for the normal development and functioning of the placenta.
- Cornelia de Lange syndrome
- Down syndrome
- Edwards syndrome
- Threat of premature termination of pregnancy
“+” An isolated increase in the level of this protein has no clinical or diagnostic significance.
MoM coefficient
After receiving the results, the doctor evaluates them by calculating the MoM coefficient. This coefficient shows the deviation of the level of indicators in a given woman from the average normal value. Normally, the MoM coefficient is 0.5-2.5 (for multiple pregnancies, up to 3.5).
These coefficients and indicators may differ in different laboratories; the level of hormone and protein can be calculated in other units of measurement. You should not use the data in the article as norms specifically for your research. It is necessary to interpret the results together with your doctor!
Next, using the PRISCA computer program, taking into account all the obtained indicators, the woman’s age, her bad habits (smoking), the presence of diabetes and other diseases, the woman’s weight, the number of fetuses or the presence of IVF, the risk of having a child with genetic abnormalities is calculated. High risk is a risk less than 1:380.
Example: If the conclusion indicates a high risk of 1:280, this means that out of 280 pregnant women with the same indicators, one will give birth to a child with a genetic pathology.
Special situations when indicators may be different.
- IVF - β-hCG values will be higher, and PAPP-A values will be lower than average.
- When a woman is obese, her hormone levels may increase.
- In multiple pregnancies, β-hCG is higher and the norms for such cases have not yet been established precisely.
- Diabetes in the mother can cause hormone levels to rise.
Help me understand the results of 1 screening. Conducted at 13 weeks. KTR 62 mm, TVP 0.1 mm, NK 3 mm. There are no minimum standards for TVP anywhere. hCGME/l, PAPP-A 1801.5 IU/l. I rewrote everything correctly. I don’t know if IU and MED are the same. First child. 35 years. Thank you in advance
Seems to be normal. The main thing is that there is a nasal bone and the TVP is no more than 3mm
Hello. Tell me with the results of 1 screening. Was at 13 weeks. Fetal heart rate - 155 beats/min, CTR - 74 mm, TVP - 2.3 mm, BPR - 21.0 mm, Chorion/Placenta - high on the posterior wall. The nasal bone is identified. HCG 166.6 IU/l, equivalent to 4.663 MoM, PAPP-A - 1.636 IU/l, equivalent to 0.338 MoM. The second child. I am 37 years old. Thank you in advance.
I have the same ultrasound. Blood is better. But they still sent me for amniocentesis. Down risk 1:69. You also need to visit a geneticist. I don't want to scare you. But everything is sad about blood((((.
Hello. My screening results are the same as yours. How is your baby?
Please tell me the results of 1 screening. I did it at 13 weeks. KTR - 66, KTR 2 - 0.00, TVP - 1.40, TVP 2 - 0.00. PAPP-A -0.40, Free hcg - 0.12 according to the life Cycle program. Astraia papp-a program - 0.44. Free hcg - 0.16. Second child, 30 years old. Thanks in advance.
Expected risk of Trisomy
Hello, please answer my question. I have a second pregnancy, 15 weeks. I recently did a blood test (screening) for Down pathology. The result: Basic risk: Trisomy 21 - 1:577 Individual. risk: Trisomy21 - 1:11549; Baseline risk: Trisomy 18 - 1:1431;
Individual risk: Trisomy:28622;
Baseline risk: Trisomy:4484;
Trisomy risk index: 89673
Hello, please help me decipher the screening results.
According to ultrasound: period 12 weeks 5 days, CTE 63.2 mm, heart rate 154 beats/min, TVP 1.60 mm, nasal bone 2.5 mm, BPR 18.1 mm, DB 9.4 mm.
According to HD: free beta subunit of hCG: 80.96 IU/l / 2.182 MoM
PARR-A: 6.777 IU/l / 2.751 MOhm
Individual risk (basic+ultrasound+BC):
Trisomy 21: 1:2621
Trisomy 18: 1:6382
Trisomy 13: 1:20026
They wrote that there were deviations in serum markers and referred me for a consultation with a geneticist.
Should I worry?
Hello. Almost identical tests, how is the baby? I'm worried too) thanks in advance. Same age at pregnancy
Hello, the first screening showed that we accept such people as cosmonauts, according to all indicators there are no deviations, but... only…. The butterfly of the brain is not symmetrical. The right hemisphere turns out to be slightly larger than the left. I'm in panic. I’m old and I’m 34 to give birth to my second one. I don’t want to give birth to a sick person. They told me to do an ultrasound at 16 and then at 20 weeks, to monitor my condition. I'm afraid it will be too late later...
Hello, please help me decipher the tests. Duration - 12 weeks 4 days. Weight 54 kg. PAPP-A 0.71 (units of measurement except the word PTO are not written before the numbers). Free hcgb- 1.62 (similar to the front only PTO). Are these indicators normal? What worries me is that I didn’t know that they would take blood and I was eating, but in response to my comment, they took everything early.
Tell me, what does this mean? hCGHME/l=2.3 MOM PARR-A 13 ng/ml=1.18 MOM e built 0.9 nmol/l= 1.76 MOM
Could this be a sign of Down syndrome?
hCG 82.17 MoM 2.585
PAPP-A 3.056 MoM 0.552
Trisomy 18: 1:2901
Trisomy 13: 1:1380
Please help me decipher the results of the first screening
RARR-A,93MoM
St. HCG 42.36 - 1.07 MoM
second pregnancy, 12 weeks, age 35 years
Hello, help me understand the result of the first screening.
Ktr 54mm. Neck fold 1.10mm. 0.77Mohm
PAPP-A 5.29 mIU/ml 1.97 MoM adj.
fb-hCG 70.8ng/ml 1.40 Accor.Mom
Biochemical risk +NT< 1:10000 ниже порога отсечки
Age risk 1:314
Trisomy 13/18 +NT<1:10000 ниже уровня отсечки
Age 34 years, first child
Good afternoon, please help me decipher the results of the first screening
fetal heart rate 152 beats/min
TVP 1.50 mm venous flow PI 1.00
Free hCG beta subunit 19.0 IU/l equivalent to 0.440 MoM
PAPP-A 2.050 IU/l is equivalent to 0.714 MoM
Trisomy 21 1:818 1:16361
Trisomy 18 1:2003<1:20000
Trisomy 13 1:6282<1:20000
pregnancy 12 weeks 6 days by ctr
Good afternoon. Yesterday I received the results of 1 screening, I am in a state of pre-shock, please help me with the answers...
My details: 39 years old, first IVF pregnancy, donor. I took ultrasound and blood tests on the same day.
Ultrasound CTR 44 (11 weeks and 2 days of pregnancy) TVP 1.7 mm, nasal bone visualized 2.8 mm, heart rate 158 beats per minute. There are no signs of pathology on ultrasound.
Blood b-hCG 109.NG/ml - 2.11 Mohm
rrr-r 2.58 med/ml - 1.39 Mohm
Biochemical risk 1:162 above the threshold cutoff
double test 1:160 above cutoff
Age risk 1:179
Trisomy<1:ниже пороговой отсечки
I read everything I could find... It seems that the ultrasound and blood readings are normal, so why are there such big risks?
Please tell me, after the 1st trimester, the ultrasound showed apparently the size of the baby I had was 13 weeks. shown size dist1 0.17 cm is this normal or not? (I’m very worried
Good afternoon Help, do they offer to undergo an expensive DNA procedure for the first screening, is it worth it or not?
28 years old, first child. 12 weeks. CTE 65.0 mm, TVP 1.6 mm, placenta set low on the wall, hCG 143.1 IU/l-3.616 MoM, PAPP-A 2.465 IU/l-0.604 MoM, trisomy 21-1:186, trisomy 18.13 is normal. The nasal bone is determined (ultrasound at 19 weeks showed 7.4 mm), ultrasound and biochemical parameters indicate a low risk of chronomomic pathology of the fetus. I had an ultrasound at 19 weeks, everything was normal. The geneticist, even after 2 ultrasounds, wrote Tr 21 threshold risk in conclusion. Is it worth getting tested, and is everything ok with the screening?
Help me figure out 12 week screening
Hello. Help me to understand. I'm 33 years old. Pregnancy2. The first screening was done at 13 weeks + 3 days. Ultrasound everything is normal. The doctor’s tests were alarming and I was referred to a geneticist. hCG 28.20 IU/l-0.833 MOM. PAPP-A 6.920 IU/l-2.227 MOM.
Hello, help me figure it out. Doctors don’t say anything. I’m 31 years old, this is my second pregnancy. The first screening was done at 12 weeks + 5 days. The ultrasound is all normal, the thickness of the collar space is 1.60 mm, the nasal bone is defined, the coccygeal-parietal size is 62.4 mm. I was referred to a geneticist. I take duphaston to maintain pregnancy 1t × 3 times a day. After this analysis, the doctor reduced the dose to 2 tablets per day, and soon we will be completely free of them. hCG 109.00 me/l -4.311 mΩ PAPP-A 1.290 m/l -0.813 mΩ. Expected risk: trisomy 21 base risk 1:519 individual risk 1:258 trisomy 18 base risk 1:1258 individual risk< 1:трисомия 13 базовый риск 1: 3948 индивидуальные риск <1:20000. объясните пожалуйста, что не так?
Do you have the size of the nasal bone?
I have similar data, the length of the nasal bones is 1.4 mm, which is small, the norm is 3 mm.
I was told that the hormones should be approximately equal, but for me there is a big difference. I am at risk, the child may have Down syndrome, a chorionic villus biopsy was prescribed
Hello, how is your baby? The tests are about the same; the free beta subunit hCG is elevated 218.20 IU/l/ 4.914 Mohm
Hello! The first screening showed everything was normal, but the hCG was 2.11 mom. What does this mean? The doctor did not decipher it for me.
Hello! Help me decipher the screening was at 11 weeks 6 days, indicators: ktr 61, heart rate 171 beats\m, TVP 1.7 mm, nasal bone 2.0 mm
Read the article above, everything is described in detail and everything is clear
hello, please help me decipher 1 screening for 13 weeks +2 days, I am 28 years old, third pregnancy, maternal serum biochemistry
free beta subunit hCG 96.17 IU/l / 2.987MoM
RPRR-A 11.690 IU/l/ 2.337 MoM
Hello! I am 25 years old, weight 56.3 kg. Please tell me if there is a risk for pathology with the following results of 1 screening at 12 days, 5 days: free beta subunit hCG 50.70 IU/l / 1.182 MoM, PPRR-A 3.870 IU/l / 1.062 MoM,
Condition Basic risk Individual risk
Trisomy 21 1:928 1:7415
Trisomy 18 1:2192<1:20000
Trisomy 13 1:6896<1:20000
Ultrasound: fetal heart rate 169 beats/min, CTE 57.0 mm TVP 2.00 mm
The nasal bone is visualized.
Doplometry of the ductus venosus: 0.88
Hello! Help me decipher the screening, please. I'm 27, weight 56.1 kg.
Term according to ultrasound is 12 weeks 5 days. PM 12 weeks 1 day.
hCGb 55.4 ng/mL 1.18
PAPP-A 3860.3 mU/L 1.19
Down syndrome 1:14903 border 1:250
Edwards syndrome 1: limit 1:100
Patau syndrome 1: limit 1:100
Turner syndrome 1: limit 1:100
Good afternoon! Help me decipher the screening. I am 23 years old. Second pregnancy. First premature!
MoM of the cervical fold - 0.92
Age risk - 1:1006
Biochemical risk T21 - 1:798
Combined risk for Trisomy: 4200
Trisomy 13/18+NT - 1:10000
Pregnancy period 12 weeks and 1 day
Hello! Can you advise me. I am 35 years old. Duration 13 weeks. Ultrasound result: KTR-78mm, heart rate-165 beats/min., TVP-1.3mm, length of the nasal bones-2.1mm. Genetic screening: Down syndrome (biochemistry) 1:102 high risk. This is the result of blood.
help me decipher, otherwise my doctor doesn’t explain anything, but simply sends me for AFP and hCG testing.
KTR-78, TVP-2.30 RAPP-A 1.65 and 1.76, Free hCG 3.18 and 3.62. Pregnancy 13.6 weeks. According to the risk calculation for Down syndrome 1:655 (according to the Astaria program 1: 2310) Edwards syndrome 1:100000 (according to the Astaria program 1:51337) Patau syndrome 1:100000 (according to the Astaria program 1:160135) Turner syndrome 1: triplondia 1:100000
Help me decipher 37 years old childbirth 3. Screening 1st trimester period 12 weeks 4 days. Heart rate 164, CTE 59.6, TVP 2, Nasal BONE determined, dopometry of the ductus venosus 0.98. HCG 13.90 MEL/0.492 MOM, PAPP-A 0.506 MEL/0.384 MOM. TRISOMY 21-1:169, trisomy 18-1:404, trisomy.
Hello! My name is Natalia, I am 39 years old. Help me decipher the 12 weeks 3 days screening. Heart rate/min, CTE - 60 mm, TVP - 1.1 mm, hCG 50.28 IU/l 1.270 MoM, PAPP-A 1.520 IU/l 0.452 MoM
Trisomy 21 - 1.86
Trisomy,650
Trisomy,510
Trisomy, 4137
Trisomy,8632
Sincerely. Waiting for an answer
Please tell me, 1st screening 12.5 days hCG readings 44.8 IU/l 1.152 Mohm
PAPP-A 0.295 IU/l 0.227 MoM. Ultrasound TVP-1.8mm KTR-78mm
Help. 28 years.
12 weeks 2 days.
The nasal bone is determined
HCG 147.4 IU/l is equivalent to 3.596 MoM
PAPP-A 2.209 IU/l is equivalent to 0.861 MoM
Trisomy 21 basic 1:781 individual 1:1023
Trisomy 18 basic 1:1843 individual<1:20000
Trisomy 13 basic 1:5799 individual<1:20000
Hello! Help me understand screening tests 1 My answers came back like this b-hCG-free 13.2 ng/ml and PAPP-A 1.8 mcg/ml
My age is 18 years old, ultrasound was done at 13+1 weeks. Heart rate - 152
HTC-64.71 IU/l/ 1.447 mOhm
Nasal bone: determined; Doppler of the triscuspid valve: regurgitation; Doppler of the ductus venosus: 1.10
Trisomy 21 Basic 1:1131individual 1:1358
Trisomy 18 basic 1:2847 individual 1:10855
Trisomy 13 basic 1:8908 individual<1:20000
Please help me decipher the results of the first screening.
Age 23, ultrasound done at 12+3 weeks.
PAPP-A 1.150 MoM (5.162 IU/L);
fb-hCG 0.840 MoM (34.25 IU/L);
Trisomy 21 ...1:20219
Trisomy 18….1:48221
Help with decoding please! First screening results:
29 years old, weight 60 and height 148 cm
Number of pregnancies: 3;
Gestation period (G) 12 weeks + 6 days according to KTR
Fetal heart rate 169 beats/min
Chorion/placenta: high on the posterior wall
Amniotic fluid: normal amount
Nose bone: determined
Free hCG beta subunit 97.1 IU/L equivalent to 3.095 MoM
PAPP-A 1.273 is equivalent to 0.487 MoM
Trisomy 21 basic risk 1:673 individual risk 1:142
Trisomy 18 basic risk 1:1652 individual risk 1:20000
Trisomy 13 basic risk 1:5179 individual risk 1:20000
How serious is it? I went to a geneticist for an ultrasound at 20 weeks(((((I’m very worried... I’m preparing myself for the worst because the geneticist said that there is a high risk of Down syndrome((((((
Good afternoon Help me understand the results of the 1st trimester screening. Heart rate 166 beats/min, CTE 50.0 mm, BPR 17.5 mm, TVP 1.20 mm, Head circumference 68.2 mm, Coolant 58.3 mm, Thigh length 6.1 mm Nasal bones are determined. I did it at 12 weeks (from the first day of menstruation). Ultrasound indicated 11 weeks and 2 days. HCG 5.606 Mohm, PAPP-A 1.266 Mohm.
Please tell me. 1 screening 12 weeks exactly ultrasound very good
HCG 35.60 MEL/0.925 MoM
PAPP-A 0.500 MEL/0.259 MoM
39 years old. They scheduled a consultation with a geneticist, but without saying anything they sent me for inactive diagnostics. I didn’t believe them, I did it in another clinic: the term is 12+6 and the real one is 13+1
HCG. 33.6ng/ml/0.35MOM
PAPp-A 1.15mlu/ml/0.80 MOM
The thickness of the collar space is 1.5 mm
Biochemical risk + NT 1:351
Age risk 1:88
Trisomy 13/18+NT 1:1894
It is now possible to do a non-invasive prenatal test. How are you doing?
Good evening! Please tell me I received a test for papp-a 0.18 mΩ and hCG 1.2 mΩ. It is written that the concentration of papp-a. Significantly reduced. The ultrasound was at 10 weeks) there are no pathologies. But analysis scares me. What to do in such a situation?
At what exact address are ultrasounds performed?
Good evening! Please tell me, analysis in the 1st trimester 12 weeks 2 days for CTE, CTE 58 mm, thickness of the portal space 1.8 mm, nasal bone is determined, biochemistry of the mother's serum Svoboda beta subunit hCG 12.48 IU/l/0.349 MoM, PAPP-A 0.487 IU/l/ 0.124 MoM, Fetal heart rate 160 beats/min, Trisomy 21 Basic risk 1:134, index risk 1:882
Trisomy 18 base risk - 1:317, index risk 1:30
Trisomy 13 base risk 1:998 index risk 1:107
Omphocele detected. Tell me how to understand all this, explain all these indicators and risks..
The risk is written low..What does this all mean?
Have you been diagnosed with omphacele?
strange results. redo it somewhere else quickly. Are you in Moscow?
Hello! I’m 43 years old, pregnant for 9 years, my daughter is 22 years old, the rest of the pregnancies were medical abortions, one of them was frozen. The pregnancy was unplanned. My last period was 10/11/16. In November, there was a delay.
Ultrasound (screening) revealed an anomaly of the uterus, class U 2a according to AFSC. Due to a septum in the uterus, we learned about pregnancy at 12 weeks. paraovarian cyst on the left, the left tube and ovary, according to the doctor, have already undergone age-related changes and do not function. Menstruation lasts 1 day on time, is painless and always “on schedule”, menstruation has been scanty for 8 years (approximately). All doctors are at a loss - with this In the set, this is 100% infertility, but so, I don’t even know what it is... On December 1, 2016, they set a period of 12 weeks. They urgently did screening: 12 weeks. 4 days. Heart rate 158 per minute, rhythmic, TVP 2.1-normal, nasal bones are located 2.6 mm, top. jaw 7.7 mm, IV ventricle 2.0 mm, reverse not registered, PI-0.77. BPR-16.1mm, No features identified.
Biochemistry on the same day: fb-hCG-60.2 ng/ml 1.46 MoM, PAPP-A-4.44 1.42 MoM
Biochemical risk +NT 1:225 above the cut-off threshold, double test 1:165-above the threshold, age-related risk 1:32 above, trisomy 13/18+NT<1:10000ниже порога отсечки.Скрининг от "ИНВИТРО".
I registered on December 7, 2016 at the antenatal clinic, showed an ultrasound, they said that the biochemistry of diagnostic (paid) centers is not taken into account, the results were only from a special institution where specialists carry out the tests (municipal, of course), they took the blood again, they didn’t do it at lunchtime on an empty stomach, etc. Until today there are no results, the deadline is running out, the brain has “exploded”. It’s scary because of my age, and I also understand that the risk is high in relation to developmental anomalies. I’m going crazy... I would be grateful for your answer .
You are at high risk solely due to age. But, this does not mean that you are at risk specifically, but simply that your age group is at risk. I think, given your story, this pregnancy is a gift from God. Keep it and you will be happy. Like now?
Good afternoon Help me understand the screening results! According to the ultrasound, everything is fine. Pregnancy 13 weeks
Markers: conc. unit. Cor. PTO
hCGb. 11.1 nh/ml. 0.34
PAPP-A. 1870.0 mU/L. 0.70
please help decipher CTE 60.0 mm. Heart rate 150.0 beats. BPR 22.0 mm. umbilical cord 3 vessels. free beta subunit hCG 133.5 me/l is equivalent to 4.249 mΩ. PAPP-A 1.448 me/l is equivalent to 0.730. trisomy 21 base risk 1:112 index risk 1//:40, trisomy 18 base risk 1:268, index risk 1:5367, trisomy 13 1:843, index risk 1:16865
Hello, help me decipher 1st screening 12 weeks 6 days: ktr 65 bpr 20 cool 63 db 10.1 heart rate 143 tvp 1.93 nasal bones visualized 1.78 and in the blood test I saw only a risk of 1:83, what should I be afraid of?
please help me decipher
Berta hCG free (mom) 11.14 weeks (1.13)
Calculate the risk of Trisomy 13/18 (including nt) 1:10000, which is a low risk value.
Neck fold mom (1.72)
Age risk (1:1014)
Biochemical risk T21(1:7157)
Combined risk for trisomy 21(1:1992)
Good afternoon, we had a screening at 13.3 weeks. Monochorionic monoamniotic twins. According to ultrasound, one child is at 13.3 weeks, the second is 12.6 weeks. CTE for the first is 72 mm, for the second is 64 mm, TVP is 2 mm, for the second is 1.9; the length of the nasal bone in the first is 2.4 mm; in the second, 1.8 mm. The choroid plexus of the lateral ventricles in the first baby is without any features, but in the second it is not clear. Sent for control after 14 days. Tell me what these results mean, the appointment is not soon, the doctor does not explain anything.
Please tell me, the first screening has been passed, all indicators are normal with the exception of PAPP-A, they are lowered, tell me, should I panic?
Elena, we have the same problem. Did anything become clear for you?
Good afternoon. Help me decipher the first screening.
Second pregnancy, I'm 30 years old. Ultrasound screening done at 12 weeks 1 day
thigh length - 8.7 mm
nose bone: determined
Collar thickness 1.8 mm
length of nasal bones 2.2 mm
blood flow in the venous duct is not disturbed Pi - 1.2
hCG: 70.12 IU/l / 1.706 MoM
PAPP-A: 1.613 IU/L / 0.439 MoM
Trisomy 21 base risk 1:637, individual risk 1:1185
Trisomy 18 base risk 1:1549, individual risk 1:30986
Trisomy 13 base risk 1:4862, individual risk 1:24111
PAPP-A: downgraded, was it worth panicking?
Good afternoon. Help decipher the results of the first screening.
Gestation period 12 weeks 6 days
Fetal heart rate 154 beats/min
The bones of the nose are determined
Free beta subunit hCG 3.29 IU/l/ 0.086 MoM
PAPP-A 0.454 IU/l/ 0.129 MoM
Age 30 years
Base risk 1:648
Ind. Risk 1:12966
Base risk 1:1592
Individual. Risk 1:89
Base risk 1:4991
Individual. Risk 1:1454
Hello, I’m 23 years old, weight 63.1st pregnancy, screening took place at 12 and 6 weeks, please decipher, I can’t find a place for myself. KTR-65.0.VP-1.20.HG-42.90 (equivalent to 1.270 MoM ),PAPP-A-1.241 (equivalent to 0.428MoM). Trisomy 21-1:040 (basic), 1:1568 (individual). Trisomy 18 1: 2555 (b) and 1: 49387 (i). Trisomy 131: 8011 (b) and 1:45899 (i). Thank you very much in advance.
I am 33 years old, weight 48 kg, 1st pregnancy, 1st fetus, had the flu at 5 weeks.
Ultrasound (at 12 weeks 0 days) - CTE 57 mm, TVP 1.1 mm, visualization of the nasal bone 1.9/1.9 mm. Ultrasound risk 1:3090
Blood (at 12 weeks and 6 days) - hCG 143 ng/ml, PAPP-A 7.64 mIU/ml. What is the risk for blood?
Is there any reason to worry about early illness?
Good afternoon! Help me figure it out! I had 1 screening done at 12 weeks and 5 days, after the ultrasound I was diagnosed at 13 weeks. I’m 30 years old and pregnant.
Fetal heart rate 158 beats/min
The nasal bones were 2.2 mm (they said they were below the norm, the norm was 2.3 mm), and they immediately sent me to donate blood.
Results: bHgch 30.94 IU/l 0.745 MoM, PAPP-A 12.410 IU/l 2.294 MoM
Trisomy 21 base: 1:632 ind.: 1:387
Trisomy 18 base: 1:1574 ind: 1:1752
Trisomy 13 base: 1:4931 ind.: 1: 20000. Help, please!
Hello! Please help me understand the screening tests for the 1st trimester.
Ktr: 68mm 13 weeks 1 day
Marker. Conc. Unit. Corr.mom
hCGb. 152.8. ng/mL. 4.46
Papp-a. 446.0. mU/L. 0.13.
Hello. I am 39 years old. I have a 17 year old son. My husband is 29 years old. At 11 weeks and 1 day, I underwent 1st trimester screening.
hCG 22.60 IU/L 0.472 MOM
PAPP-A 1.060 IU/L 0.629 MOM
Trisomy 21 base risk 1:84; individual risk 1:1675
Trisomy 18 base risk 1:188; individual risk 1:3767
Trisomy 13 base risk 1:595; individual risk 1:11898
They referred me to a geneticist. The geneticist insists on invasive examination. Help me to understand.
please tell me if my test is normal?
PAPP-A 1 5.40 mIU/ml
β-HCG (free β-HCG) 21.18
β-HCG (free β-HCG) (MOM) 0.59
termweek weight 57kg 29 years
Hello, help me figure it out, I’m 38, second pregnancy. FETAL heart rate is 154 beats/min. CTE is 75.0 mm. TVP 2.10mm. Nasal bone is determined. Free beta subunit of hCG 21.70 IU/l /0.673MoM. PAPP-R: 13.190 IU/l /2.648MoM. Trisomy21. base risk 1:126. Individual 1:2524. Trisomy 18 base risk 1:324. individual 1:6483 Trisomy 13 base risk 1:1012. individual<1:20000
How to determine the normality of tests?
Fetal heart rate 158 beats/min, CTE 75 mm, TVP 1.5 mm, nasal bone 1.9 mm determined, Free beta unit 71.32 IU/l / 2.657 MoM, PaPP-A 5.286 IU/l / 1.235. Duration 13 weeks. and 4 days
I’m 37, my first pregnancy, long-awaited by screening: CTE 75.0; TVP1.40; BPR 22.9; OG 87.0 According to ultrasound without pathologies, but the blood: HCG 1.397 MoM; PAPP-A 0.244MoM. They put a high risk of trisomy 21-1:41. They sent me for a non-invasive prenatal DNA test. This test will show you exactly whether there are other tests. The puncture is not indicated for me due to hereditary thrombophilia. (I inject Fraxiparine)
Hello! Help with sorting out the tests: 3rd pregnancy. 30 years
ultrasound 1st trimester 05/16/2017 (estimated pregnancy period 10 weeks 4 days)
fetometry: CTE 48 mm. embryo size = 11 weeks. 5 days
nasal bone 2.2 mm.
general screening: from 05/17/2017 (calculated by ultrasound 11 weeks 5 days)
rrr- A=0.53 MOM. HCG-3.12 MOM
Disease Down Syndrome
Age risk 1:810………..Calculated risk 1:184 -High risk
Disease Down Syndrome only in biochemistry
Age risk 1:810………..Calculated risk 1:28 -High risk
Other indicators are low risk.
Question...what week is the calculation based on? At 10 and 12 weeks then the tests will be normal, if at 11 weeks then yes there are risks of increased hCG...
Converted MOM to another unit (ng/ml)…using medians
Which week should I take for calculation? if 1 day of last menstruation. 03/03/2017
Good afternoon. Help me understand the screening results.
Ultrasound and blood tests 12 weeks 5 days
Fetal heartbeat: determined, heart rate 166 beats/min. PI:0.91
Collar thickness: 1.6mm
Nasal bone visualized: 2.1mm
Bones of the calvarium: b/o
Brain structures: M-echo: b/o
Anterior abdominal wall: b/o
Choroid plexuses: b/o
IV ventricle: Four-chamber section of the heart: b/o
Bladder: used
Upper and lower limbs: b/o
Yolk sac: not visible
Amnion: features: b/o
Predominant localization of the villous chorion: posterior wall of the uterus, thickness 13 mm
Orion structure: b/o
Condition of the uterine walls: b/o
Ovaries: right corpus luteum 23mm
Conclusion: Ultrasound signs of progressing pregnancy, 13 weeks
Blood test data:
PRISCA I trimester test
Pregnancy-associated protein A (PAPP-A): 0.95 mIU/ml
Free b-subunit 26.40ng/ml
Hello. Help me figure it out. Pregnancy 14 weeks. Free beta subunit 18.50 IU/l 0.568 MoM. PAPP - A 0.667 IU/l 0.193. Trisomy 21 1:471 and Trisomy 18 1:122. What will the geneticist say?
Good afternoon I ask for your advice.
2nd pregnancy, 13 weeks. and 3 days. 40 years. Weight 70.4. By ultrasound and blood:
KTR 72 mm, BPR 22 mm, LZ 29 mm, OG 82 mm, coolant 71 mm, femur length 11 mm. Heart rate 158.
TVP 2.1 mm. The nasal bones are visualized, 2.6 mm.
The thickness of the chorion is 19 mm, along the posterior wall of the uterus. An interstitial-subserous myomatous node with a diameter of 47 mm is located along the posterior wall of the uterus. Hypertonicity of the myometrium along the anterior wall of the uterus.
Free beta subunit of hCG 23.30 IU/l/0.658 MoM.
PAPP-A 2.170 IU/l/ 0.616 MoM.
Baseline risk: trisomy:69. Trisomy: 174. Trisomy: 545.
Individual. risk of trisomy:827. Trisomy: 3486. Trisomy: 2476.
34 years. Fourth pregnancy. 1- caesarean. 2 - miscarriage. 3 - frozen. And here is the 4th: 1st trimester screening at x 18 risk 1:67, at x 135 risk 1:136. Panic-hysteria!! The gynecologist referred me to a geneticist, but immediately warned me that piercing would be prescribed and most likely termination of pregnancy. I followed the diet only the day before the test, and even then not on the doctor’s recommendation, but on my own. The doctor didn’t warn about anything except about the test on an empty stomach (but even a fool can understand that)) Who had these or similar indicators? What's the result?
Hello, who can help decipher the first trimester screening results?
30 years old, weight 67 kg, 2nd pregnancy
according to ultrasound - 11 weeks 5 days: CTE 50 mm, TVP 2.7 mm, heart rate 185 beats/min
blood - 12 weeks 0 days: fb-hCG 59.8 ng/ml (1.45 Adj.MoM), PAPP-A 4 mlU/ml (1.86 Adj.MoM).
Biochemical risk+NT 1:386 (below cut-off)
Double test 1:4893 (below the cutoff)
Age risk 1:576
Trisrmia 18+NT less than 1:10000 (below the cut-off threshold)
Hello, please tell me. I had a 1st trimester screening. 12 weeks. Enzyme immunoassay. Study of the level of protein associated with pregnancy in the blood 6.563 mlu/ml 2.47MOM. And a study of the level of human chorionic gonadotropin in the blood is 49.14 lu/ml 1.42MOM. Did the ologist send you to a perenatologist? Tell me what this means. And what threatens me there according to the tests?
Add a comment Cancel reply
Do you know everything about colds and flu?
© 2013 ABC of Health // User Agreement // Personal Data Policy // Site Map The information on the site is intended for informational purposes only and does not encourage self-treatment. To establish a diagnosis and receive treatment recommendations, consultation with a qualified physician is necessary.
With Doppler ultrasound, it is possible to obtain CSC from the superior and inferior vena cava, ductus venosus, hepatic veins, pulmonary veins, and also umbilical veins. The most studied vessels are the inferior vena cava (IVC) and the ductus venosus (DV). The curve of blood flow velocity from the inferior vena cava, obtained by studying its segment located immediately distal to the junction with the ductus venosus, is characterized by a three-phase profile.
First antegrade wave corresponds to ventricular systole(SG), the second antegrade wave of a smaller size - early ventricular diastole, and the third, characterized by the reverse direction of blood flow, corresponds to the phase of atrial systole (AS). Various indices have been proposed for the analysis of FCS in the IVC, but our recent studies have demonstrated that the assessment of the preload index is more effective than others described in the literature for predicting the threatening condition of the fetus.
This index expressing relationship between maximum speed venous blood flow in the phase of atrial systole and its maximum speed in the phase of ventricular systole (Preload Index (A/S) = SP /SF), depends on the pressure gradient between the right atrium and the right ventricle at the end of diastole, which is a reflection of both the diastolic function of the ventricles, and the level of end-diastolic pressure in them.
Visualization of the venous duct is possible with a cross section of the upper abdomen of the fetus at the level of its origin from the umbilical vein. Then the Color Doppler mode is turned on, and the control volume of the pulsed wave Doppler is set slightly above the area of entry of the venous duct (closer to the umbilical cord vein) - at the point where the maximum blood flow velocity is recorded during Color Doppler. Its CSCs are characterized by a biphasic nature, with the first peak corresponding to ventricular systole (wave S), the second to ventricular diastole (wave D), and the lowest blood flow velocity is observed during atrial systole (incisura A).
Among the proposed indexes To quantitatively characterize the SSC in the venous duct, the angle-independent S/A ratio between the maximum velocities in ventricular systole (S) and atrial systole (A) turned out to most effectively reflect its hemodynamics.
The type of SSC of the hepatic veins is similar the same in the NPV. There are a few studies in the literature devoted to the study of blood flow in these vessels in the fetus, however, given the data presented in them, it can be argued that analysis of blood flow in the hepatic veins can be as informative as in the IVC.
KSK of pulmonary veins examined in the area of their entry into the right atrium. The appearance of the resulting curves will also be characterized by antegrade blood flow during the phase of atrial contraction. Identification of marked changes in the nature of blood flow in the IVC and pulmonary veins is of particular interest, since this may reflect the state of hemodynamics in the systemic and pulmonary venous circulation during intrauterine development of the fetus.
blood flow in the umbilical cord vein is usually continuous. However, if there is reverse blood flow in the IVC during the phase of atrial contraction in the umbilical cord vein, a pulsating nature of the CSC may be observed. During the normal development of pregnancy, this kind of pulsation is observed only up to 12 weeks and is a reflection of the rigidity of the ventricular walls in this gestational period, which determines the high frequency of reverse blood flow in the IVC.
In later stages of pregnancy recording the pulsating nature of blood flow in the umbilical cord vein will be a sign of severe cardiac dysfunction.
Return to the contents of the section " "
The child has a violation of uterine blood flow. It was diagnosed as grade 3a. Term 27 weeks. They said they would look at my blood flow every 3 days. If something happens, the child 800 grams will not survive and if something happens he will not be healthy. I'm losing my mind. My indicators for blood flow are 3.11 Pi in the artery above the norm 1.61 PI in the mate artery on the left 1.56 above the norm 2.20 above the norm on the right. PI in the cerebral artery the norm is 2.32 Ultrasound from 7.11 uzist another PI pulsation index absent in the umbilical cord artery. Pi on the left is 2.01.
Doppler: the essence of the method, implementation, indicators and interpretation
It is impossible to imagine an area of medicine where additional examination methods would not be used. Ultrasound, due to its safety and informativeness, is especially actively used in many diseases. Doppler measurements are an opportunity not only to assess the size and structure of organs, but also to record the features of moving objects, in particular, blood flow.
Ultrasound examination in obstetrics provides a huge amount of information regarding the development of the fetus; with its help, it has become possible to determine not only the number of embryos, their gender and structural features, but also to observe the nature of blood circulation in the placenta, fetal vessels and heart.
There is an opinion that examining expectant mothers using the ultrasound method can harm the unborn baby, and with Doppler ultrasound the radiation intensity is even higher, so some pregnant women are afraid and even refuse the procedure. However, many years of experience in using ultrasound allows us to reliably judge that it is absolutely safe, and such a quantity of information about the condition of the fetus cannot be obtained by any other non-invasive method.
All pregnant women should undergo Doppler ultrasound in the third trimester; if indicated, it may be prescribed earlier. Based on this study, the doctor excludes or confirms a pathology, the early diagnosis of which makes it possible to begin treatment in a timely manner and prevent many dangerous complications for the growing fetus and mother.
Features of the method
Doppler measurement is one of the ultrasound methods, so it is carried out using a conventional device, but equipped with special software. It is based on the ability of ultrasound waves to reflect from moving objects, thereby changing their physical parameters. Reflected ultrasound data is presented in the form of curves that characterize the speed of blood movement through the vessels and chambers of the heart.
The active use of Doppler ultrasound has become a real breakthrough in the diagnosis of almost all types of obstetric pathology, which is usually associated with circulatory disorders in the mother-placenta-fetus system. Through clinical observations, indicators of norms and deviations were determined for various vessels, which are used to judge a particular pathology.
Doppler testing during pregnancy makes it possible to determine the size and location of blood vessels, the speed and characteristics of blood movement through them at the moment of heart contraction and relaxation. The doctor can not only objectively judge the pathology, but also indicate the exact location of its occurrence, which is very important when choosing treatment methods, since hypoxia can be caused by pathology of the uterine arteries, umbilical vessels, and disturbances in the development of fetal blood flow.
Doppler testing can be duplex or triplex. The latter option is very convenient because not only the speed of blood flow is visible, but also its direction. With duplex Doppler, the doctor receives a black-and-white two-dimensional image, from which the machine can calculate the speed of blood movement.
example of a triplex Doppler examination frame
Triplex examination is more modern and provides more information about blood flow. The resulting color image shows blood flow and its direction. The doctor sees red and blue streams on the monitor, but to the average person it may seem that this is arterial and venous blood moving. In fact, the color in this case does not indicate the composition of the blood, but its direction - towards or away from the sensor.
No special preparation is required before Doppler ultrasound, but the woman may be advised not to eat or drink water for a couple of hours before the procedure. The examination does not cause pain or discomfort; the patient lies on her back, and the abdominal skin is treated with a special gel that improves ultrasound performance.
Indications for Doppler testing
Ultrasound with Doppler as a screening is indicated for all pregnant women in the third trimester. This means that even in the absence of pathology, it should be carried out as planned, and the obstetrician-gynecologist will definitely refer the expectant mother for examination.
The optimal period is considered to be between 30 and 34 weeks of pregnancy. At this time, the placenta is already well developed, and the fetus is formed and gradually gaining weight, preparing for the upcoming birth. Any deviation from the norm in this period is clearly visible, and at the same time, doctors will still have time to correct the violations.
Unfortunately, not every pregnancy proceeds so well that the expectant mother undergoes an ultrasound with Doppler measurements on time and, rather, for prevention. There is a whole list of indications for which the study is carried out outside the established framework for screening and even more than once.
If there is reason to suspect fetal hypoxia or a delay in its development, which is noticeable with conventional ultrasound, then a Doppler study will be recommended within a week. Before this period, it is not advisable to carry out the procedure due to the insufficient development of the placenta and fetal vessels, which can cause erroneous conclusions.
Indications for unscheduled Doppler testing are:
- Diseases in the mother and pathology of pregnancy - gestosis, kidney disease, high blood pressure, diabetes mellitus, Rh conflict, vasculitis;
- Fetal disorders - developmental delay, oligohydramnios, congenital malformations of organs, asynchronous development of fetuses in multiple pregnancies, when one of them is significantly behind the others, aging of the placenta.
Additional Doppler testing of the fetus may be indicated if its size does not correspond to what it should be at this stage of pregnancy, because slower growth is a sign of possible hypoxia or defects.
Other reasons for performing an ultrasound with Doppler may include an unfavorable obstetric history (miscarriages, stillbirths), the age of the expectant mother over 35 years or under 20, post-term pregnancy, entanglement of the umbilical cord around the fetal neck with the risk of hypoxia, changes in the cardiotocogram, damage or trauma to the abdomen.
Doppler parameters
When performing an ultrasound with Doppler, the doctor assesses the condition of the uterine arteries and umbilical cord vessels. They are most accessible to the device and well characterize the state of blood circulation. If there are indications, it is possible to assess blood flow in the baby’s vessels - the aorta, middle cerebral artery, kidney vessels, and heart chambers. Typically, such a need arises when certain defects are suspected, such as intrauterine hydrocephalus or developmental delay.
The most important organ that unites the body of the mother and the unborn baby is the placenta. It brings nutrients and oxygen, while simultaneously removing unnecessary metabolic products, realizing its protective function. In addition, the placenta secretes hormones, without which the proper development of pregnancy does not occur, so without this organ the maturation and birth of a baby is impossible.
The formation of the placenta begins virtually from the moment of implantation. Already at this moment, active changes in blood vessels occur, aimed at sufficiently supplying the contents of the uterus with blood.
The main vessels supplying blood to the body of the growing fetus and the enlarging uterus are the uterine and ovarian arteries, located in the pelvic cavity and in contact with each other in the thickness of the myometrium. Branching into smaller vessels in the direction of the inner layer of the uterus, they turn into spiral arteries that carry blood to the intervillous space - the place where the exchange of blood between the mother and baby occurs.
Blood enters the fetal body through the vessels of the umbilical cord, the diameter, direction and speed of blood flow in which are also very important, primarily for the growing organism. Possible slowing of blood flow, reverse flow, abnormalities in the number of vessels.
Video: series of lectures on fetal circulation
As the gestational age increases, the spiral vessels gradually expand, and specific changes occur in their walls, allowing a large volume of blood to be delivered to the ever-growing uterus and baby. The loss of muscle fibers leads to the transformation of arteries into large vascular cavities with low wall resistance, thereby facilitating the exchange of blood. When the placenta is fully formed, the uteroplacental circulation increases approximately 10 times.
With pathology, proper transformation of blood vessels does not occur, the penetration of trophoblast elements into the uterine wall is disrupted, which certainly entails pathology in the development of the placenta. In such cases, there is a high risk of hypoxia due to lack of blood flow.
Hypoxia is one of the most powerful pathogenic conditions, under which both growth and differentiation of cells are disrupted, therefore, during hypoxia, certain disorders on the part of the fetus are always detected. To exclude or confirm the fact of lack of oxygen, Doppler ultrasound is indicated, assessing blood flow in the uterine, umbilical vessels, and intervillous space.
example of hypoxia due to impaired placental blood flow
The ultrasound machine records so-called blood flow velocity curves. For each vessel they have their own limits and normal values. The assessment of blood circulation occurs throughout the entire cardiac cycle, that is, the speed of blood movement in systole (contraction of the heart) and diastole (relaxation). For data interpretation, it is not the absolute blood flow indicators that are important, but their ratio in different phases of the heart.
At the moment of contraction of the heart muscle, the blood flow rate will be the highest - maximum systolic velocity (MSV). When the myocardium relaxes, blood movement slows down - end-diastolic velocity (EDV). These values are displayed as curves.
When deciphering Doppler data, several indices are taken into account:
- Systole-diastolic ratio (SDR) is the ratio between the end-diastolic and maximum blood flow velocity at the time of systole, calculated by dividing the MVR by the CDS;
- Pulsatility index (PI) – from the MSS indicator we subtract the KDS value, and divide the resulting result by the average speed (SS) of blood movement through a given vessel ((MSS-KDS)/SS);
- Resistance index (RI) - the difference between systolic and diastolic blood flow is divided by the MSS index ((MSS-KDS)/MSS).
The results obtained can either exceed the average normal values, which indicates high peripheral resistance from the vascular walls, or decrease. In both cases, we will be talking about pathology, because both narrowed vessels and dilated ones, but with low pressure, do an equally poor job of delivering the required volume of blood to the uterus, placenta and fetal tissues.
In accordance with the obtained indices, three degrees of disorders of the uteroplacental circulation are distinguished:
- At grade 1A, an increase in IR in the arteries of the uterus is detected, while blood flow in the placental-fetal part is maintained at a normal level;
- the opposite situation, when blood circulation is impaired in the vessels of the umbilical cord and placenta, but preserved in the uterine arteries, is characterized by 1B degree (IR is increased in the umbilical cord vessels and normal in the uterine ones);
- In grade 2, there is a disorder of blood flow both from the uterine arteries and placenta, and in the vessels of the umbilical cord, while the values have not yet reached critical figures, the DPT is within normal limits;
- Grade 3 is accompanied by severe, sometimes critical, values of blood flow in the placental-fetal system, and blood flow in the uterine arteries can be either altered or normal.
If Doppler testing reveals the initial degree of circulatory disorders in the mother-placenta-fetus system, then treatment is prescribed on an outpatient basis, and after 1-2 weeks the pregnant woman needs a repeat ultrasound with Doppler to monitor the effectiveness of therapy. After 32 weeks of gestation, multiple CTG are indicated to exclude fetal hypoxia.
Impairment of blood flow of 2-3 degrees requires treatment in a hospital with constant monitoring of the condition of both the woman and the fetus. At critical values of Doppler measurements, the risk of placental abruption, intrauterine fetal death, and premature birth increases significantly. Such patients undergo Doppler measurements every 3-4 days, and cardiotocography is performed daily.
Severe disturbance of blood flow, corresponding to grade 3, threatens the life of the fetus, therefore, in the absence of the possibility of its normalization, the question of the need for delivery is raised, even if this has to be done ahead of schedule.
Premature artificial birth in some cases of pathological pregnancy is aimed at saving the life of the mother, because intrauterine fetal death due to inadequate blood flow can cause fatal bleeding, sepsis, and embolism. Of course, such serious issues cannot be resolved by the attending physician alone. To determine tactics, a council of specialists is created that takes into account all possible risks and possible complications.
Norm and pathology
Since the state of the blood vessels of the uterus, placenta, and fetus constantly changes throughout pregnancy, it is important to evaluate blood circulation precisely by correlating it with a specific gestational age. For this purpose, average norms have been established for weeks, compliance with which means normality, and deviation means pathology.
Sometimes, if the condition of the mother and fetus is satisfactory, some deviations are detected during Doppler testing. There is no need to panic, because timely diagnosis will allow you to correct the blood flow at a stage when changes have not yet caused irreversible consequences.
Weekly norms involve determining the diameter of the uterine, spiral arteries, umbilical cord vessels, and fetal middle cerebral artery. The indicators are calculated starting from week 20 and up to 41. For the uterine artery, IR within a week is normally no more than 0.53. gradually decreasing towards the end of gestation, in a week it is no more than 0.51. In spiral arteries, on the contrary, this indicator increases: outside the week it is no more than 0.39, by the 36th week and before birth - up to 0.40.
Fetal blood flow is characterized by the umbilical cord arteries, the IR for which does not exceed 0.79 until the 23rd week, and by the 36th week it decreases to a maximum value of 0.62. The baby's middle cerebral artery has similar normal resistance index values.
SDO during pregnancy gradually decreases for all vessels. In the uterine artery, the intraweek indicator can reach 2.2 (this is the maximum normal value), by the 36th week and until the end of pregnancy it is no more than 2.06. In spiral arteries, SDO was no more than 1.73, in 36 – 1.67 and lower. The umbilical cord vessels have an SDO of up to 3.9 by 23 weeks of gestation and no more than 2.55 at one week. In the baby's middle cerebral artery the numbers are the same as in the umbilical cord arteries.
Table: SDO norms for Doppler measurements by week of pregnancy
Table: summary values of norms of planned Doppler measurements
We have given only some normal values for individual arteries, and during the examination the doctor evaluates the entire complex of vessels, correlating the indicators with the condition of the mother and fetus, CTG data and other examination methods.
Every expectant mother should know that ultrasound with Doppler ultrasound is an integral part of the entire pregnancy monitoring period, because not only the development and health, but also the life of a growing organism depends on the condition of the blood vessels. Careful monitoring of blood flow is the task of a specialist, so it is better to entrust the decoding of the results and their interpretation in each specific case to a professional.
Doppler measurements not only allow for timely diagnosis of severe hypoxia, gestosis in the second half of pregnancy, and delayed fetal development, but also significantly helps prevent their occurrence and progression. Thanks to this method, the percentage of intrauterine deaths and the frequency of severe complications during childbirth in the form of asphyxia and neonatal distress syndrome have decreased. The result of timely diagnosis is adequate therapy for pathology and the birth of a healthy baby.
Basal temperature from A to Z
BeTeshka is your assistant in pregnancy planning
1 screening, Blood flow in the venous duct Pi=0.98 how to decipher?
Girls, please tell me what these Pi = 0.98 mean!?
Yesterday I had my first screening, here are the results:
The thickness of the collar space is 1.5mm
The nasal bone is visualized 2.8
Bones of the calvarium 23
Thigh length 10.8
Blood flow in the ductus venosus Pi =0.98
Chorion localization: anterior, structure unchanged
Everything is clear to me, except for the venous duct, can anyone tell me? The doctor said nothing, didn’t even answer anything (And the uzist didn’t even show the baby(
Read 10 comments:
In the conclusion of the 1st screen, I don’t have anything like that at all, it just says that the blood flow in the TC is normal, I don’t know what the TC is. Don't bother. I think if there was something wrong, the ultrasound specialist or doctor would definitely tell you about it
nezhnov4ik, Thank you, but they are not particularly friendly doctors, everything is somehow silent. I'm not worried, I'm just very interested, I can't find the transcript))))))
YuliyaT, I think this is just an indicator of blood flow
This is not written in my report either. If there was something wrong, the doctor and ultrasound specialist would have told me about it. So don't worry
Raccoon, we persuaded you)) I won’t go on the Internet to look for information anymore)))
added less than a minute ago
YuliaT, I have in my report) pi-0.851, but I didn’t even attach any importance to it, since the doctor said that everything is fine))) don’t worry
They didn’t write this for me either, but I found something on the Internet, there’s a table there
In general, you were done with Doppler measurements
edited less than a minute ago
added after 3 minutes
Uterine artery pulsation index PI, table 2, by week
added after 10 minutes
It’s true that starting from the 20th week (perhaps until the 20th week the PI simply does not change) and it is clear that with each week the PI decreases, but it seems that everything is fine with you, especially since they didn’t say anything.
cassiopea777, so I’m not the only one who has this meaning)))) thank you.
added after 2 minutes
inch, I read it, it’s very interesting, now I understand why they did Doppler testing for me, I have diabetes, apparently they insure themselves, and me too) thank you.
Yes, blood flow is monitored after 20 weeks. Don't bother yourself. Healthy big baby)
Leave a comment:
You must register or log in to be able to comment.
- Build a graph:
- Registration
- Remind password
- Information:
- Registered: people
- BT schedules: pcs.
- FAQ on working with charts
- Rules on BeTeshka
- Search for "Yasha" and Search for "Gosh"
- Help in deciphering gr. BT
- Help for newbies
- AzBuka BeTeshki for beginners
- Blog of communication between planners
- “Pregnant” BT charts
- Our rulers
- Contacts
- Sections:
- Sandbox (35)
- Basal temperature (5184)
- Planning a pregnancy (8882)
- Reproductive technologies (IVF, ICSI, AI) (427)
- Pregnancy (4372)
- Childbirth (1005)
- Children (1640)
- Health (3407)
- Specialist consultations (337)
- Reviews about doctors (364)
- Reviews about clinics (medical institutions) (11)
- Personal diaries (1220)
- Faith and Religion (156)
- Competitions and promotions (297)
- Holidays and travel (136)
- Our meetings (15)
- Review of foreign online stores (27)
- Hobbies and leisure (265)
- Handmade (handmade goods) (77)
- Congratulations (2280)
- Geography of BeTeshka (216)
- Alcove (6669)
- Medicines: buy/sell/give away (102)
- Basket (5573)
- Administration messages (123)
- list of sections
- Add a review about your doctor
- How did you get to BeTeshka?
- Recipes with photos
- 20 facts about me, let's get closer to each other
- Our photo gallery!
- “Weight loss” Let's lose weight together!
- Charity on BTashka
- BTshki Award 2017!
- Quiz! “What we were, what we became-2”
New blog topics:
- Pregnancy planning:
- On line: Visitors: 98
Registered: 31, guests 67.
Use of materials only with the permission of the administration, subject to an active link to the site.
uziprosto.ru
Encyclopedia of Ultrasound and MRI
Doppler examination of the fetus, indicators and norms
Modern medicine is constantly evolving. This is especially true for the development of research methods. And this lies largely not in the emergence of new methods, but in the development of existing ones and the expansion of their application.
Over the past decades, the ultrasound research method has significantly expanded its scope and range of diagnostic capabilities. The development of the Doppler method and elastography allows not only to assess the structure of the area under study, but also to assess the function based on data on the blood supply to the area of interest.
Ultrasound examination in obstetrics is used relatively recently, but is the main screening method. The history of the use of Doppler in fetal examination goes back about 25 years. During this time, enough information and experience have accumulated, on the basis of which it can be argued that this method helps in diagnosing a large number of pathologies and choosing the right pregnancy management plan.
Doppler method
Assessment of the fetal condition using Doppler ultrasound is based on the dependence of fetal parameters on blood flow in the feeding vessels and their speed parameters. The speed of blood flow in the vessels under study depends on a number of factors: the type of vessels and their elastic properties, blood pressure, and the volume of circulating blood. Deviation of speed parameters from the established norm may be a sign of fetal pathology, dysfunction of the uteroplacental circulation.
The method is based on the effect described by Doppler at the end of the 19th century. It was formulated as a law of optics and acoustics, but has found wide application in medicine, in particular in ultrasound research. In obstetrics, devices whose operation is based on the Doppler effect are: fetal heartbeat detectors, cardiotocographs, ultrasound diagnostic devices with Doppler function.
In ultrasound, this effect is used in two forms: color Doppler mapping (CDC) and blood flow velocity curves. With the help of color flow, the presence of blood flow and its direction are determined from warm and cold flows. KSK allows you to determine the maximum systolic and end-diastolic velocities, the resistance index.
Conducting research
Doppler examination of the fetus is performed during ultrasound diagnostics if indicated. All modern devices used for ultrasound examinations of pregnant women have this function. For a pregnant woman, a Doppler ultrasound examination is no different from a regular examination; it does not require special preparation, but may take longer.
Doppler examination of a pregnant woman
During diagnosis, the doctor determines blood flow rates and resistance indices in the vessels being examined. The scope of Doppler diagnostics of the fetus is individual and depends on the indications. This is due to the fact that this type of diagnosis requires the use of more power, and this, in turn, leads to stronger heating of the tissue. At the present time, there is not enough data to confirm the negative impact of Doppler on the fetus and the course of pregnancy, but this does not exclude their presence. Therefore, diagnostics must be carried out according to indications and to the required extent.
Research results and norms
Uterine arteries
Due to the fact that these arteries are not visualized with conventional ultrasound in B-mode, the search for vessels occurs using color circulation. It is necessary to determine the resistance index for CSC. Doppler examination should be carried out on both sides, since most often dysfunction of the uteroplacental blood flow is unilateral.
Norms of resistance indicator in the uterine arteries
The most common reason for an increase in the resistance index is a violation of trophoblast invasion. In pathology, the values of this indicator are very variable and can differ significantly from each other even after short time intervals.
Umbilical arteries
Determining blood flow in the umbilical arteries, its speed and resistance index is quite difficult and routine. The method requires experience and compliance with a number of conditions to obtain correct results.
To conduct the study correctly, you must:
- the use of a frequency filter should be minimal
- measurement should be carried out with minimal fetal movements, heart rate should not exceed 160 beats/min.
- the measurement is carried out 4-5 times, the average value is taken as the true value (variability of no more than 10% is considered optimal)
- to determine blood flow indicators, the middle section of the umbilical arteries is selected
- The optimal angle for Doppler measurements is considered to be up to 45º, but values up to 60° are acceptable
- The study is carried out with the pregnant woman lying on her back.
Norms for IR at different stages of pregnancy
In the second and third trimester, there is a noticeable decrease in the resistance of the umbilical arteries. This occurs due to increased growth of the terminal branches of the umbilical arteries and increased blood flow in the chorionic villi. When the uteroplacental blood supply decreases, the maximum diastolic blood flow velocity decreases and, accordingly, the resistance index increases.
A persistent decrease in uteroplacental circulation causes intrauterine growth retardation. Diagnosis of this condition is very important, since a critical increase in IR (against the background of the absence of diastolic blood flow or the presence of reverse diastolic blood flow) for 2 weeks leads to fetal death in all cases.
Aorta
The study of the aorta and blood flow indicators is best carried out in the thoracic region, before the departure of large branches. Determination of Doppler indicators in the aorta is carried out within a period of weeks or later. This is due to the fact that in the first trimester of pregnancy, the speed parameters in the aorta do not change even in the presence of pathology, since its compensatory capabilities are high. At the same time, changes in indicators in the aorta are a more specific and diagnostically important criterion due to the fact that they reflect the degree of hypoxia and hemodynamic disturbances in the fetus itself.
In the absence of pathology, with increasing gestational age, the resistance index changes slightly, but the blood flow speed increases.
Doppler norms in the fetal aorta
Gestation period, weeks. Pulsatility index (PI) Resistance index (RI) Average blood flow velocity, cm/s
Middle cerebral artery
Blood flow in the middle cerebral artery in a fetus with hemolytic disease, Dopplerogram
The study of blood flow in this artery is often of an applied nature. To identify the artery, color circulation is used, followed by Doppler measurements. Normally, in the second and third trimesters of pregnancy, there is a gradual decrease in the vascular resistance index and an increase in the average blood flow velocity.
With fetal hypoxia, centralization of blood circulation occurs, which leads to an increase in velocity indicators in the cerebral arteries and, accordingly, a decrease in the resistance index. An increase in the resistance index may be a sign of intracerebral hemorrhage.
Doppler norms in the cerebral artery
Ductus venosus
This vessel is a continuation of the umbilical vein inside the fetal body. The vessel is easily identified in B-mode during conventional ultrasound examination. There are no established generally accepted norms of blood flow and indices for the ductus venosus. To identify pathology, they focus on zero and reverse indicators of blood flow in diastole.
The type of blood flow in the venous duct is of practical importance in cases of intrauterine development disorders and heart defects. Often, Doppler testing of this vessel is performed dynamically in case of developmental delay and allows one to decide on the issue of prolonging pregnancy or emergency delivery.
In addition to studying blood flow in the main vessels, Doppler ultrasound is widely used for intrauterine Doppler echocardiography. This high-tech method is the main one for intrauterine detection of heart defects in the fetus.
The high information content of Doppler testing is undeniable, but it should be taken into account that this method should not become a screening method. Of course, there is no reliable data on the negative impact of Doppler testing on a pregnant woman and unborn child, but the volume of research should be determined individually and not exceed the minimum required level.
Indications for Doppler sonography are:
- on the part of a pregnant woman - toxicosis, pathology of the kidneys, cardiac system and blood vessels
- on the part of the unborn child - intrauterine growth retardation, suspicion of heart and vascular defects
- features of the course and pathology of pregnancy - multiple pregnancy, polyhydramnios, oligohydramnios, untimely aging of the placenta
- burdened obstetric history - non-developing pregnancy, intrauterine fetal death, intrauterine growth retardation during previous pregnancies.
Ductus venosus pulsation index is normal
Golubitox for diabetes. Official website.
How to determine this type of diabetes? It is necessary to take so-called stress tests, when sugar is determined not only on an empty stomach, but also after eating a high-carbohydrate meal (usually sugar syrup is used as such) - the sugar in this test should not exceed 10 mmol/l. Order Golubitox for a promotion - [link-1] - read reviews 95% of patients demonstrated a stable decrease in blood sugar, regardless of diet; By the third week of taking the tincture, 67% reduced the amount.
Lymphatic system.
What is lymph? The fluid contained in the blood (plasma) passes through the walls of the capillaries and penetrates the tissues. Now it is interstitial fluid. It seeps into the intercellular spaces, nourishes the cells and takes away some of the toxic products of their vital activity. In the interstitial fluid there is an accumulation of metabolic products - ions, fragments of disintegrated lipids, fragments of destroyed cells. Part of the interstitial fluid is collected by the veins, the rest is excreted by the lymphatics.
Along the path of the vessels there are lymph nodes - oval, 0.3-3 cm in size, formations, passing through which the lymph is freed from harmful substances and pathogens and is enriched with lymphocytes, i.e., it performs one of the barrier functions of the body.
Lymphatic vessels merge into trunks, and subsequent ones into lymphatic ducts. In this case, from most of the body, lymph collects into the left thoracic duct (length 30-45 cm), which flows into the left venous node (the junction of the left subclavian and internal jugular veins), and from the upper right part of the body - into the right lymphatic duct, which flows into right subclavian vein.
Is it possible to detect oncology at the preclinical stage?
How to prevent the development of oncology at the preclinical stage, and therefore before the appearance of complaints and manifestations, or make sure that you are out of danger? Specially developed programs of the Treatment Center will help you with this. The programs are aimed at diagnosing and monitoring therapy for prostate, testicular, ovarian, cervical and endometrial cancer, pancreatic, gallbladder, bile duct, stomach, liver, intestinal and lung cancer. “ONCORISK - Laboratory assessment of cancer risk.
If you're that smart. About yours, about your girl’s
Very often you want to tell people if you are so smart. then why are you: -poor -lonely -unhappy Why do shoemakers without boots most often give sound advice?
I took a test for hemostasis + VA + D-Dimer. Pregnancy and childbirth
Girls, good afternoon! I’m the reader who brought up the topic about varicose veins NOT on my legs. I thought and thought and went to get tested in the morning. Here are the results, I was upset for some reason, the doctor told her to call only in the evening, she understands, I’m starting to get a little worried :)) Fibrinogen concentration - 5.8 (normal 1.8-6.0) APTT - 32 (20-40) Prothrombin index (80-125) r+k - 10+8=18 (19-27) ma - 55 (40-52) ITP - 15.3 (6-12) Platelet aggregation ADP (50-75) RKMF - negative ( negative) D-Dimmer.
Vera, talk to several doctors. For some reason, everyone is very wary of thromboass. Tomorrow they promised to find out the opinion of another doctor. About chimes - I decided to drink it, I’ll drink it for 21 days, then we’ll see. About Wobenzym. I don’t know, we’ll see, there’s no tone right now.
By the way, here are some more tips:
Try not to stand or sit - it’s better to walk and lie down briskly. If you sit, then sit on a soft ball (there are such huge ones).
Do exercises. This is why I really want to take the course. If I find out, I’ll tell you about it in case it’s useful to someone else.
Very good swimming. Honestly, we have a swimming pool on Krasnogvardeyskaya, but I’m really squeamish or something. They promised to find out about the pool on Chertanovskaya - I’ll also write what and how. There’s some kind of water there - I forgot, either artesian, or mischievous. In general, I’ll find out and write.
Help. Other children
Hello! I want to ask for help. First, I will describe the situation: My close friend has a growing daughter, she is 2 years old. Almost 3 months ago she was diagnosed with meningoencephalitis. She had a high fever. She was bitten by a tick, it is not clear whether she was bitten or not, but as her grandmother says, she complained about the bite. She was admitted to the hospital in intensive care and was connected to a ventilator. 2 months ago one could say that she was on the mend. They turned off the device and came to my senses. They were transferred to.
First screening, listeriosis, etc. just to you.)). Pregnancy.
Hi all. I’ve been reading you for a long time, I’m writing anonymously too)))))) Today I finally had an ultrasound and I want to officially join your company!))))) Health, health and once again health to everyone!! It's hard to do without questions. 🙂 1) At the first screening ultrasound, what did they look at? Only the CTE, the place of attachment, the collar were named - and that’s it. Fingers and inner They don't look at the organs yet, right? Because I have an LCD, haven’t they messed with it? 2) The test for listeriosis came back awesome - I was found to have antibodies to it.
1. coccygeal-parietal size of the fetus
2. biparietal size of the fetus
3. fetal heart rate
4. presence of a yolk sac (may no longer be visualized)
5. Bones of the vault of the skull
6. fetal spine
7. anterior abdominal wall
8. Bladder
9. new bones
11. fetal limbs
13. ductus venosus of the fetus (I don’t know, maybe they don’t look in the gastrointestinal tract)
14. location of the chorion, structure of the chorion
But all this was looked at in the cir and given out in the description. In LCDs they probably also look at the same things, they just talk about fewer parameters. There, for screening, they almost only write CTE. So don't worry about this.
I won’t say anything about listeriosis; I’ve never even heard of such a thing. But if you are confused by the infectious disease specialist in the regiment, ask for a referral to 1 infectious disease hospital (it is located on Volokolamsk Highway). The doctors there are very competent; after all, they work with infections every day. And the housing complex should give directions there free of charge. In general, although it’s scary to go to an infectious diseases clinic, it’s better to go there where you can figure it out correctly than to just go to the clinic. But there’s nothing scary there, everything is very nice.
Fetal heartbeat - please tell me. Planning a pregnancy
Girls, you know a lot of things here and what you understand, maybe you can tell me something. I am in the 7th week of my period, ovulation was late - the actual period is the 4th week. A week ago, an ultrasound scan diagnosed a detachment, yesterday they said that the detachment seemed to be getting better, but the heartbeat - they saw something (either the baby’s heart, or my pulse), 105 beats per minute. The good doctor said that it would be better if it were my pulse: 0(, because if it’s a baby’s pulse, then there’s a direct path to us. You know where, but it’s normal.
Do an ultrasound in a GOOD place. A GOOD doctor.
What they told you smacks of illiteracy.
If there are problems, then you need to know about it, and not “either SB or pulse”
1) For experienced doctors, it is almost impossible to make a mistake (whose pulse is). I saw with my own eyes: you can see such an oval darkening there - a fertilized egg and it is pulsating. Yes, it is difficult to calculate (there is a big error there), but whose pulse is wrong?
2) At your term SB this is too much. Usually.quite acceptable. For example, for me (in the embryo) it was 110. By the way, due to detachment, SB may actually decrease slightly. Up to 100 is acceptable.
Where is a good neurologist in Moscow? Other children
I posted it in a separate topic. I decided not to inject celebrozilin yet, but to show the girl to several more doctors. Tell me, who?
Mommy is upset, listen to advice like Cheroke! We, too, after one very “competent specialist”, developed the usual dislocation of the shoulder, and now we are struggling to put support on our hands, and the dislocation is very disturbing: ((And if the sound of the joint popping out has already appeared, then under no circumstances should you put pressure on these places exercises that lead to such a sound - each crack is accompanied by abrasion of the heads of the joints, be sure to draw the attention of your massage therapist and exercise therapy instructor to this. You must definitely allow the joints to strengthen naturally, but this does not mean that you should not work with them at all, but simply choose the right exercises for their development.
They did a Doppler. Venous dysfunction.. Other children
Today we did a Doppler test at Nevromed. Conclusion: venous dysfunction. She didn’t explain anything, she said that all questions should be addressed to a neurologist. Tell me what this could be and what to do next? Or is this no longer curable?
Polyhydramnios. How to deal with this? Pregnancy and childbirth
I had an ultrasound today (Thank you everyone for your support!). The doctor immediately said that my stomach was big, and I could feel it myself. As a result, they diagnosed me with polyhydramnios. I didn’t have this in my last pregnancy, so I don’t know at all what the risk is and whether anything can be done about it. Tomorrow I’ll see a doctor, but I’d like to know the experience of those who are familiar with this. Thank God, everything is fine with the little one! It’s just that the placenta is still a little low, but I hope that it will rise.
The fontanel is pulsating. A child from birth to one year
It’s something I haven’t seen before, but now it’s visible to the naked eye. It's been probably two weeks now. I spoke with a neurologist, she was silent for a long time, asked questions and prescribed Diacarb for 3 days and Asparkam. I trust her very much, she pulled Katya out for me. But she didn’t say that, she said we’ll talk in 3 days. But I’m somehow tense. I don’t even want to go on the Internet, now I’ll read too much and won’t sleep at all. You better tell me, is this very scary?
Mild throbbing pain? Pregnancy and childbirth
Hello, I am 6 weeks pregnant, and my lower abdomen periodically pulls in my stomach, but not too much. I went to the doctor and he said everything was fine, but I was still a little worried about it. Sometimes I feel a slight throbbing pain in the lower abdomen, on the side. It doesn't hurt me, but I'm very afraid that something might be wrong. Could you tell me if this might be normal. I mean that slight throbbing pain. Maybe someone had the same thing?
From right to left there is a sipping, tingling sensation - normal, not scary. The main thing is to listen to yourself and don’t worry. In addition, the doctor also confirmed that there were no concerns. So everything will be fine! Take care of yourself and your belly!
Induction of labor without indications. Pregnancy and childbirth
Almost a horror story, but knowing is better than not knowing. The recent increase in the number of patients with cerebral palsy indicates that the number of birth injuries has increased. This is directly related to the use of labor stimulation. Birth stimulants began to be used abroad from the early 50s, and in Russia - from the early 60s. It was from this time that there was a sharp increase in the number of children with cerebral palsy. During childbirth, physiological (i.e. normal) processes occur in close proximity.
Questions have appeared. Planning a pregnancy
Girls, I had a question after a conversation with my husband :) We saw a man with a stitch after surgery - it goes straight across the stomach, and goes around the navel in an arc, and straight again. I suggested that in this case the navel could be removed and the seam should be made exactly in the center (aesthetically, the stomach is already ruined anyway), but my husband says that this is not possible, that something important should remain there from birth, and it is needed. And here’s the question: after cutting the umbilical cord, what happens to the baby’s blood vessels? How do they disappear? Where.
The blood flow of the ductus venosus is impaired. Pregnancy and childbirth
What does it mean? They wrote in the conclusion of an ultrasound scan at 12.5 weeks. And not a word about it at the reception. Everything else is normal. Maybe someone had a similar experience, please tell me.
Strange pulsation of the uterus. Pregnancy and childbirth
Pregnancy 33 weeks. For quite some time now I have been worried about a strange pulsation of the uterus (or contractions). Approximately 30 times per minute, lasting 3-4 times a day (a bit like vaginal contractions after orgasm, only in the uterus). Maybe someone knows if this is normal. I asked different doctors, including when I was being kept in the maternity hospital. They don't attach any importance to it. They say the baby hiccups. But it doesn't look like hiccups at all. I have also been worried about hypertension since 22 weeks.
How much to pay a nurse for intramuscular injections at home.
Just don’t drive me to the “health”, because there are few visitors there, and the nurse will come at lunchtime, you need to decide how much money to give her. 50? 100? Our syringes. An additional condition is that the promotion is not a one-time event; injections will have to be done weekly for at least a year. You can’t go to the clinic, there are no neighbors who are skilled, you haven’t learned how to do it yourself yet:((Tell me something worthwhile. Thank you.
GV and temperature. Breast-feeding
Girls, can the temperature just rise to 37.7 during breastfeeding? I have no signs of a cold, but one nipple is cracked until it bleeds: (Perhaps there is an infection there? What is it anyway? The child’s breasts are completely empty, there is no congestion or lumps, should I see a doctor?
Waist size and illness. User's blog PoLe on 7ya.ru
Pregnancy: first and second screening - assessing the risks.
Screening during pregnancy - pros and cons. Ultrasound, blood test and additional studies.
I have already encountered the incompetence of our doctors more than once!
My sister couldn’t have children for 9 years, and finally, thanks to IVF, she became pregnant at the age of 41. Everyone was incredibly happy. The doctor in the residential complex said right off the bat - like where should you give birth to an old child. Plus, after 1 screening on Friday before the weekend, I called in the evening and said that congratulations - you will be born Down 👿 👿 👿 👿 The poor thing cried all weekend, they couldn’t calm me down, my friends advised take a prenatal test (yes, it cost a lot - they paid 29,500 rubles), but they said it was effective. And in 5-6 days you can find out for sure whether there is a pathology or not.
You can’t even imagine what these 5 days were like for us. My sister, out of nervousness, ended up in the hospital with a threat. She was delivered on time.
After 5 days the result came; The baby is healthy - no pathologies have been identified.
Male fetus.
My husband almost killed this doctor at the antenatal clinic. He wanted to sue her.
Dear expectant mothers, there is no need to panic because of incompetent doctors.
After this story, when I became pregnant, I did not undergo screening.
I had an ultrasound and am planning to go straight to a prenatal test on Friday. Out of harm's way.
Children's heart. Childhood diseases
Causes of heart murmurs in children. Features of the cardiovascular system in children
Pregnancy in women with heart defects. Strategy.
Pregnancy in women with cardiovascular diseases
It consists of four departments. These are the right atrium and right ventricle, which make up the right heart, and the left atrium and left ventricle, which make up the left heart. Oxygen-rich blood coming from the lungs travels through the pulmonary veins into the left atrium, from there into the left ventricle and then into the aorta. Venous blood enters the right atrium through the superior and inferior vena cava, from there into the right ventricle and further through the pulmonary artery into the lungs, where it is enriched with oxygen and again enters the left atrium. A heart defect is a persistent pathological change in the structure of the heart that impairs its function. Heart defects can be congenital or acquired. Congenital heart defects are much less common than acquired ones.
The second hospitalization is during the week of pregnancy to monitor the state of the cardiovascular system and, if necessary, to maintain heart function during the period of maximum physiological stress. This is due to the fact that it is during this period that the load on the heart normally increases significantly (one of the periods of maximum physiological stress) - the so-called cardiac output increases by almost a third, mainly due to an increase in heart rate. Third hospitalization - this week to prepare for childbirth and choose a method of delivery, drawing up a birth plan. When a sign appears.
Heart secrets. Heart defects in children. First visit to the doctor
It is impossible to talk about all congenital heart defects in one article; there are about 100 of them. Let’s focus on the most common ones. These include patent ductus arteriosus and ventricular septal defect. Patent ductus arteriosus This is a vessel connecting the aorta (a large vessel that arises from the heart and carries arterial blood) and the pulmonary artery (a vessel that arises from the right ventricle and carries venous blood to the lungs). Normally, a patent ductus arteriosus exists in utero and should close within the first two weeks of life. If this does not happen, they say there is a heart defect. The presence or absence of external manifestations (shortness of breath, tachycardia, etc.) depends on the size of the defect and its shape. There may be external manifestations noticeable to the mother.
"Reconnaissance" without invasion. Non-invasive antenatal methods.
Prenatal screening. Prenatal diagnosis. Pregnancy examinations
Therefore, with a probability of%, developmental defects can be excluded. Some dimensions are also measured: the length of the bony part of the dorsum of the nose (this week the norm is from 6 to 9.2 mm - according to domestic authors and from 6 to 10.4 mm - according to foreign data), BPR (biparietal size), fronto-occipital size, circumference of the head, abdomen, length of the femur and humerus, bones of the lower leg and forearm. In addition to these measurements, be sure to pay attention to the shape of the nose, forehead, upper and lower jaws, etc. For example, the presence of a depression in the bridge of the nose (in combination with a number of other signs) may indicate.
First ultrasound. Ultrasound during pregnancy
What is checked at the first ultrasound during pregnancy?
I am 8 weeks pregnant. At this stage, ultrasound revealed the presence of one fertilized egg and two equal corpora lutea in it (at different “ends” of the egg), but the heart rate was only one beat. Tell me, is there any statistical data on what is the probability of two embryos developing if neither I nor my husband had twins in our family?
The cycle is irregular, on average 31 days, range from 28 to 45. The first day of the last menstruation is 04/23/2008, the previous one is 03/25/2008.
Unprotected sex took place from 4.05 to 9.05. There was no sex either before or after this period.
05/28/2008, obstetric period 5 weeks 1 day - bhCG 14224. Ultrasound result - internal dimensions of the ovum 11x5x8, the embryo is not visualized, the yolk sac is not visualized, the myometrial tone is increased.
06/04/2008 obstetric period 6 weeks 1 day. The embryo and yolk sac are visible on ultrasound. CTE 11 mm, diameter of the ovum 30*27 (I forgot the third size, because the results were not given to me). According to ultrasound, the due date is 7 weeks (which, according to my calculations, cannot be).
And most importantly, the heartbeat cannot be heard or viewed.
My question is: how far along am I actually pregnant? Can the embryo be larger than normal at my term? How likely is an error in the diagnosis of doctors!
Help please, I'm all exhausted already!
Neither more nor less. How much amniotic fluid is needed?
During external examination, parts of the fetus are clearly identified, heart sounds are heard, and the uterus is dense. A more accurate determination of the severity of oligohydramnios is possible with ultrasound examination. The diagnosis of oligohydramnios by ultrasound is based on determining the amount of amniotic fluid and on calculating the amniotic fluid index (AFI), which is automatically calculated by the ultrasound machine after measuring the amount of fluid in several places. The amount of amniotic fluid is considered normal if the IAF value is between 5 and 8 cm; An AFI of 2 to 5 cm is regarded as moderate oligohydramnios, an AFI of less than 2 cm is regarded as severe oligohydramnios. Doppler study of blood flow in the “mother - placenta - fetus” system, which is carried out.
Elements of amniotic fluid can be detected when examining vaginal discharge; the so-called amniotest is the most effective and fastest method for diagnosing premature rupture of membranes, based on the determination of placental protein in the vaginal discharge. Normally, this protein is not present in vaginal discharge. If the flow of water is significant, the woman feels discomfort from the fact that her underwear periodically becomes wet from the water. If leakage of amniotic fluid (premature rupture of the membranes) is detected during a premature pregnancy, the woman must be hospitalized in a separate room, bed rest and mandatory health monitoring.
The beat of life. Monitoring the fetal heartbeat.
This distinguishes the fetal heart from the adult heart. These structural features of the heart ensure that oxygen reaches all organs and systems of the fetus. After the baby is born, the oval window closes and the ductus arteriosus collapses. Ultrasound (ultrasound) and echocardiography (echocardiography) are used to assess fetal cardiac activity. Auscultation (listening) of the fetus, CTG (cardiotocography). Ultrasound of the fetal heart Early in pregnancy, the fetal heartbeat can be determined using ultrasound (ultrasound). Normal with transvaginal ultrasound (introducer probe.
By listening to the fetal heart sounds, the obstetrician determines their rhythm: the tones can be rhythmic, that is, they occur at equal intervals of time, and arrhythmic (non-rhythmic) - at unequal intervals. Arrhythmic tones are characteristic of congenital heart defects and intrauterine hypoxia (oxygen deficiency) of the fetus. The nature of the tones is also determined by hearing: clear and dull heart sounds are distinguished. Clear tones are heard clearly and are normal. Deafness of tones indicates intrauterine hypoxia. The fetal heartbeat may be difficult to hear if: the placenta is located on the anterior wall of the uterus; polyhydramnios or oligohydramnios; excess thickness of the anterior abdominal wall in obesity; multiple births; increased motor skills.
Can you already see it? Ultrasound in the first trimester of pregnancy.
In this case, the size of the fertilized egg is 2-4 mm. The embryo is determined from the 5th week of pregnancy during a TV study and from the 6th - during a TA study in the form of a white linear formation in the cavity of the fetal egg. At the same time or a little later, heart contractions can be determined. Normally, in the presence of a regular menstrual cycle, it is necessary to determine the presence of an embryo in the fertilized egg at 6 weeks of pregnancy using a TV scan. It is not necessary to do an ultrasound at this time, but if it is performed (at the woman’s request, in case of recurrent miscarriage), then at 6 weeks the embryo should be detected. And if the cycle is irregular, then the period of menstruation cannot be accurately determined. Then the period is determined by ultrasound and, if there is no embryo, they are looked at again. If any is detected, it is rejected.
Hormone tests. Medicine and health
Please advise. I have many, many extra pounds. I want to go on a diet. Before this, I would like to check my hormonal levels. Has anyone come across what hormones need to be checked if you are overweight? There are so many of them. I want to come to the endocrinologist with ready-made tests. Thanks Lena
1) Body mass index = Body weight (kg) / height (in meters) squared (2 degrees) The norm for a woman is 18.5 - 24.9
2) The distribution of fatty tissue is assessed by the ratio of waist circumference to hip circumference - WC/HR. The Android distribution of fat corresponds to a high WC/TB ratio - more than 0.83 for women. A high value of this coefficient indicates the development of metabolic complications of obesity (cardiovascular diseases, type 2 diabetes, arterial hypertension, hyperlipidemia, insulin resistance)
3) Blood pressure
5) X-ray of the skull
6) Laboratory research:
Fasting glucose level
Gamma glutamate transferase activity
LDL and HDL cholesterol levels
Apoprotein B and uric acid levels
Hormones (LH, FSH, prolactin, testosterone, Estradiol (E 2), TSH and free T4.
3. Gynecological examination
Sometimes, with abdominal obesity, symptoms similar to the manifestations of hypercortisolism are observed. In such patients, the daily rhythm of cortisol secretion and the excretion of free cortisol in urine are additionally examined and a small test with dexomethasone is performed.
1 check the function of the thyroid gland - take tests for free T4 and T T G
2 exclude insulin resistance - measure your waist (in women it should not exceed cm), measure fasting C peptide, make a sugar load/sugar curve
3 check with a gynecologist - rule out polycystic disease
4 check morning cortisol, ACTH
©, 7ya.ru, Certificate of registration of mass media El No. FS.
Reprinting messages from conferences is prohibited without indicating a link to the site and the authors of the messages themselves. Reproduction of materials from other sections of the site is prohibited without the written consent of ALP-Media and the authors. The opinion of the editors may not coincide with the opinion of the authors. The rights of authors and the publisher are protected. Technical support and IT outsourcing are provided by KT-ALP.
7ya.ru - information project on family issues: pregnancy and childbirth, raising children, education and career, home economics, recreation, beauty and health, family relationships. The site hosts thematic conferences, blogs, ratings of kindergartens and schools, articles are published daily and competitions are held.
If you find errors, problems, or inaccuracies on the page, please let us know. Thank you!